
Range of Motion after Dual Mobility Total Hip Arthroplasty: Does Femoral Head Size or Surgical Approach Matter?
Amgad M. Haleem, MD¹·²; Mohamed S. Gobba, MD²; Morteza Meftah, MD³; Sabir Ismaily, BS⁴; Ronald J. Mitchell, MD⁵; Philip C. Noble, PhD⁴; Stephen J. Incavo, MD⁵
¹Department of Orthopedic Surgery, Oklahoma University School of Medicine; Oklahoma City, OK, USA²Department of Orthopedic Surgery, Cairo University School of Medicine; Cairo, Egypt³Department of Orthopaedics, New York University, Hospital for Joint Disease; New York, NY, USA⁴Institute of Orthopaedic Research and Education; Houston, TX, USA⁵Department of Orthopaedic Surgery, Houston Methodist; Houston, TX, USA
Corresponding Author:Stephen J. Incavo, MD, Houston Methodist Orthopedics & Sports Medicine, 6445 Main St., Outpatient Center, Suite 2500, Houston, TX 77030, USA; sjincavo@houstonmethodist.org
DOI: 10.18600/toj.020102
INTRODUCTION
Dual mobility total hip arthroplasty (DM-THA) was developed by Gilles Bousquet in 1975. The procedure is a modification of the original Charnley concept to reduce postoperative dislocation in primary total hip arthroplasty (THA) [1]. Based on large-diameter effective head concept, it consists of a tripolar design. The prosthetic metal head is mobile in a large retentive polyethylene (PE) bearing, able to move freely in a polished metal-backed cup [2]. The first motion occurs between the inner metal femoral head and PE bearing; the secondary motion occurs between the PE bearing and acetabular cup. This design is intended to reduce the risk of dislocation by minimizing prosthetic neck impingement. This decrease in impingement occurs by increasing the head-neck ratio, with a subsequent increase in range of motion (ROM) before impingement and dislocation. Other theoretical advantages include an increased “jump distance”, which is the vertical or inferior head displacement required for dislocation, compared to a traditional large femoral head with a resultant increase in prosthetic joint stability [3].
There is abundant literature showing the efficiency of DM-THA in reducing postoperative dislocation in primary and revision THA [4-16]. Similarly, large femoral head (32 mm and larger) THA has been used to increase head-neck ratio. Large femoral heads have shown excellent functional outcomes and reduced dislocation rates [17-20]. Despite abundant literature reporting outcomes of DM-THA and large diameter conventional THA for dislocation, there is a paucity of independent (nonindustry) basic science and clinical studies reporting in vitro and in vivo ROM following implantation of these 2 distinct types of prostheses [21,22]. While the effective head size is larger in DM-THA compared to large femoral head THA, it is still unknown whether DM-THA has any superiority to conventional large femoral head THA designs in terms of postoperative ROM and subsequent improvement in function, which could translate into higher clinical outcome scores.
The effect of surgical approach after THA has also been a point of debate as it relates to hip ROM. The posterolateral (PL) approach violates the gluteus maximus and can potentially affect hip extension after THA. Conversely, the modified Hardinge anterolateral (AL) approach violates the anterior aspect of the hip abductors, thus having the potential to affect the flexion and abduction moments. While some studies have found that surgical approach has no effect on postoperative gait mechanics after THA [23-25], few reports exist on THA postoperative ROM via different surgical approaches [24,26,27].
This study aimed to test the following hypotheses: 1) DM-THA provides superior active hip ROM compared to large-diameter, 36 mm-head THA (36-THA) as measured by dynamic radiography; 2) DM-THA provides superior functional scores compared to 36-THA as evidenced by Harris Hip Score (HHS), Oxford Hip Score, and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC); 3) a posterolateral versus modified Hardinge anterolateral has an effect on postoperative hip ROM. We hypothesized that THA patients who were operated on via posterolateral approach (THA-PL) would have superior hip flexion, while THA patients operated on via modified Hardinge anterolateral approach (THA-AL) would have superior hip extension. MATERIALS & METHODS
The Institutional Review Board at the investigators’ institution approved this prospective case-control study. Written consent was obtained for all participating patients.
Data Collection
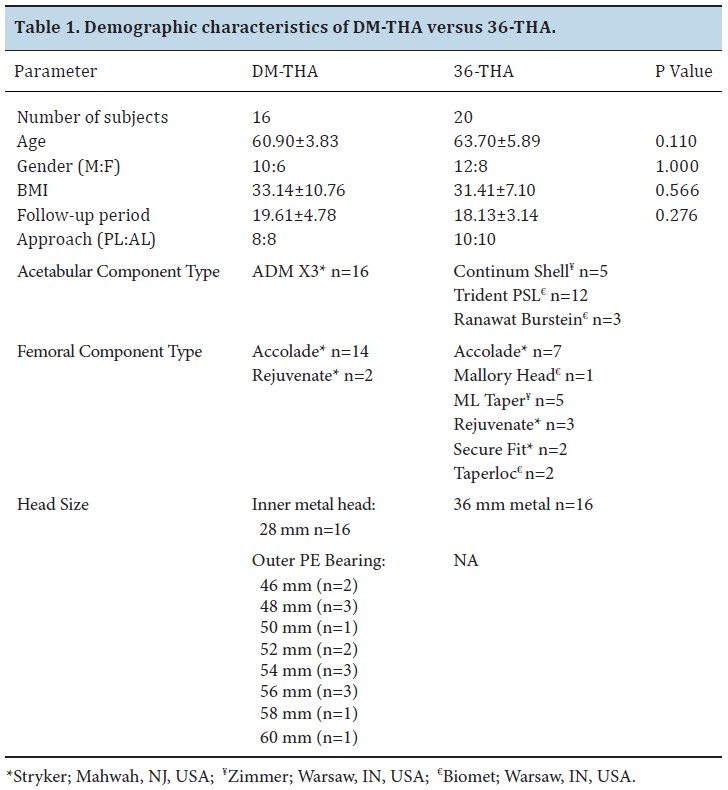
Following IRB approval, a prospective cohort of patients was identified from medical records of the senior author’s practice. These patients had DM-THA (ADM, Stryker; Mahwah, NJ, USA) through a PL or AL approach, with a minimum follow-up of 1 year. Inclusion criteria comprised patients between 25 and 90 years who had no mental/physical co-morbidities or reading disabilities to prevent them from answering functional questionnaires or obtaining required radiographs. Sixteen patients (10 males, 6 females, mean age 60.90±3.82 years) with unilateral DM-THA were identified, constituting the study group (DM-THA). Of these 16 patients, 8 (5 males, 3 females) had a DM-THA through a PL approach (DM-THA-PL), while 8 (5 males, 3 females) had a DM-THA through a modified AL approach (DM-THA-AL). The DM-THA group was matched in terms of age, sex, and body mass index (BMI) to a control group of patients who had undergone 36-THA through a PL or AL approach with the same minimum follow-up period and inclusion criteria. Twenty patients (12 males, 8 females, mean age 66.20±8.65 years) were identified. Of these patients, 10 (6 males, 4 females) had a 36-THA through a PL approach (36-THA-PL), while 10 (6 males, 4 females) had a 36-THA through a modified AL approach (DM-THA-AL). Study demographics, control groups, and a description of each subset of patients and implants are listed in Table 1. In addition to clinical functional outcome scores (HHS, Oxford, and WOMAC hip scores), lateral view standing plain radiographs of the lumbosacral spine (LSS), pelvis, and operated hip were obtained for all patients using GE DefiniumTM 8000 digital radiography machine (General Electric; Fairfield, CT, USA). X-rays were acquired in 3 different positions: standing with both hips in neutral position (neutral view), standing with maximum active hip flexion of the operated hip (flexion view), and standing with maximum active hip extension of the same hip (extension view). For neutral view, the patient stood with the operated hip opposing the film cassette, both arms supported, and pelvic rotation adjusted so that both anterior superior iliac spines (ASIS) were coplanar (Figure 1A). The X-ray beam source was placed at a distance of 180 cm and centered on the iliac crest, taking care to ensure optimum superimposition of both ASIS in all views, including the upper border of L3 vertebra to the lower LSS, pelvis, femoral heads, and the proximal femoral diaphysis. For the flexion view, the patient was asked to actively flex the operated hip maximally with careful attention to maintain the femoral shaft, patella, and foot facing directly forward to avoid compensatory rotation of the hip. Next, adjustable platforms were placed under the patient’s foot to maintain this position while acquiring the radiographic flexion view. Similarly, the extension view was taken while the patient actively extended the operated hip maximally while standing (Figures 1B,C).
Dual mobility total hip arthroplasty (DM-THA) was developed by Gilles Bousquet in 1975. The procedure is a modification of the original Charnley concept to reduce postoperative dislocation in primary total hip arthroplasty (THA) [1]. Based on large-diameter effective head concept, it consists of a tripolar design. The prosthetic metal head is mobile in a large retentive polyethylene (PE) bearing, able to move freely in a polished metal-backed cup [2]. The first motion occurs between the inner metal femoral head and PE bearing; the secondary motion occurs between the PE bearing and acetabular cup. This design is intended to reduce the risk of dislocation by minimizing prosthetic neck impingement. This decrease in impingement occurs by increasing the head-neck ratio, with a subsequent increase in range of motion (ROM) before impingement and dislocation. Other theoretical advantages include an increased “jump distance”, which is the vertical or inferior head displacement required for dislocation, compared to a traditional large femoral head with a resultant increase in prosthetic joint stability [3].
There is abundant literature showing the efficiency of DM-THA in reducing postoperative dislocation in primary and revision THA [4-16]. Similarly, large femoral head (32 mm and larger) THA has been used to increase head-neck ratio. Large femoral heads have shown excellent functional outcomes and reduced dislocation rates [17-20]. Despite abundant literature reporting outcomes of DM-THA and large diameter conventional THA for dislocation, there is a paucity of independent (nonindustry) basic science and clinical studies reporting in vitro and in vivo ROM following implantation of these 2 distinct types of prostheses [21,22]. While the effective head size is larger in DM-THA compared to large femoral head THA, it is still unknown whether DM-THA has any superiority to conventional large femoral head THA designs in terms of postoperative ROM and subsequent improvement in function, which could translate into higher clinical outcome scores.
The effect of surgical approach after THA has also been a point of debate as it relates to hip ROM. The posterolateral (PL) approach violates the gluteus maximus and can potentially affect hip extension after THA. Conversely, the modified Hardinge anterolateral (AL) approach violates the anterior aspect of the hip abductors, thus having the potential to affect the flexion and abduction moments. While some studies have found that surgical approach has no effect on postoperative gait mechanics after THA [23-25], few reports exist on THA postoperative ROM via different surgical approaches [24,26,27].
This study aimed to test the following hypotheses: 1) DM-THA provides superior active hip ROM compared to large-diameter, 36 mm-head THA (36-THA) as measured by dynamic radiography; 2) DM-THA provides superior functional scores compared to 36-THA as evidenced by Harris Hip Score (HHS), Oxford Hip Score, and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC); 3) a posterolateral versus modified Hardinge anterolateral has an effect on postoperative hip ROM. We hypothesized that THA patients who were operated on via posterolateral approach (THA-PL) would have superior hip flexion, while THA patients operated on via modified Hardinge anterolateral approach (THA-AL) would have superior hip extension. MATERIALS & METHODS
The Institutional Review Board at the investigators’ institution approved this prospective case-control study. Written consent was obtained for all participating patients.
Data Collection
Following IRB approval, a prospective cohort of patients was identified from medical records of the senior author’s practice. These patients had DM-THA (ADM, Stryker; Mahwah, NJ, USA) through a PL or AL approach, with a minimum follow-up of 1 year. Inclusion criteria comprised patients between 25 and 90 years who had no mental/physical co-morbidities or reading disabilities to prevent them from answering functional questionnaires or obtaining required radiographs. Sixteen patients (10 males, 6 females, mean age 60.90±3.82 years) with unilateral DM-THA were identified, constituting the study group (DM-THA). Of these 16 patients, 8 (5 males, 3 females) had a DM-THA through a PL approach (DM-THA-PL), while 8 (5 males, 3 females) had a DM-THA through a modified AL approach (DM-THA-AL). The DM-THA group was matched in terms of age, sex, and body mass index (BMI) to a control group of patients who had undergone 36-THA through a PL or AL approach with the same minimum follow-up period and inclusion criteria. Twenty patients (12 males, 8 females, mean age 66.20±8.65 years) were identified. Of these patients, 10 (6 males, 4 females) had a 36-THA through a PL approach (36-THA-PL), while 10 (6 males, 4 females) had a 36-THA through a modified AL approach (DM-THA-AL). Study demographics, control groups, and a description of each subset of patients and implants are listed in Table 1. In addition to clinical functional outcome scores (HHS, Oxford, and WOMAC hip scores), lateral view standing plain radiographs of the lumbosacral spine (LSS), pelvis, and operated hip were obtained for all patients using GE DefiniumTM 8000 digital radiography machine (General Electric; Fairfield, CT, USA). X-rays were acquired in 3 different positions: standing with both hips in neutral position (neutral view), standing with maximum active hip flexion of the operated hip (flexion view), and standing with maximum active hip extension of the same hip (extension view). For neutral view, the patient stood with the operated hip opposing the film cassette, both arms supported, and pelvic rotation adjusted so that both anterior superior iliac spines (ASIS) were coplanar (Figure 1A). The X-ray beam source was placed at a distance of 180 cm and centered on the iliac crest, taking care to ensure optimum superimposition of both ASIS in all views, including the upper border of L3 vertebra to the lower LSS, pelvis, femoral heads, and the proximal femoral diaphysis. For the flexion view, the patient was asked to actively flex the operated hip maximally with careful attention to maintain the femoral shaft, patella, and foot facing directly forward to avoid compensatory rotation of the hip. Next, adjustable platforms were placed under the patient’s foot to maintain this position while acquiring the radiographic flexion view. Similarly, the extension view was taken while the patient actively extended the operated hip maximally while standing (Figures 1B,C).
.jpg)
Digital radiographic data created on the workstation were imaged on the Picture Archiving and Communication System (PACS) and exported for analysis on commercially available software (TraumaCad®, BrainLab; Munich, Germany).
Maximum clinical active hip flexion and extension (thigh-trunk motion) are affected by degeneration of the LSS besides contributions from spinopelvic motion, which occurs at the level of the LSS motion segment and the sacropelvic (SP) motion segment (ie, the sacroiliac articulation) [28,29]. Therefore, contributions from both LSS and SP motion segments to clinical hip motion (thigh-trunk motion) observed on flexion and extension views were calculated and subtracted from thigh-trunk measurements in neutral, quantifying true hip joint flexion, extension, and total true hip joint ROM.
Three measurements were calculated on the neutral, flexion, and extension radiographic views using the TraumaCad software: 1) clinical hip ROM (thigh-trunk angle), defined as the angle between the vertical and a line bisecting the femoral shaft diaphysis (thigh-trunk ROM = true hip joint ROM + LSS motion + SP motion); 2) LSS lordosis angle (LSS-LA), defined as the angle between a line parallel to the upper border of L3 vertebral body and another line parallel to the upper border of S1; 3) sacropelvic angle (SP), defined as the angle between a line parallel to the upper border of S1 and another line representing the anterior pelvic plane (Lewinneck plane) [30], which is defined by a line tangent to the pubic symphysis and both ASIS. Clinical hip flexion, or the change in thigh-trunk angle flexion, was represented by the difference in thigh-trunk angle from neutral to flexion. Clinical hip extension, or the change in thigh-trunk angle extension, was calculated as the difference in thigh-trunk angle from neutral to extension. The difference in LSS-LA from neutral to flexion (the change in LSS-LA flexion) and from neutral to extension (the change in LSS-LA extension) was also calculated. Finally, the change in SP flexion was calculated as the difference in SP from neutral to flexion. The change in SP extension was the difference in SP from neutral to extension.
Three measurements were calculated on the neutral, flexion, and extension radiographic views using the TraumaCad software: 1) clinical hip ROM (thigh-trunk angle), defined as the angle between the vertical and a line bisecting the femoral shaft diaphysis (thigh-trunk ROM = true hip joint ROM + LSS motion + SP motion); 2) LSS lordosis angle (LSS-LA), defined as the angle between a line parallel to the upper border of L3 vertebral body and another line parallel to the upper border of S1; 3) sacropelvic angle (SP), defined as the angle between a line parallel to the upper border of S1 and another line representing the anterior pelvic plane (Lewinneck plane) [30], which is defined by a line tangent to the pubic symphysis and both ASIS. Clinical hip flexion, or the change in thigh-trunk angle flexion, was represented by the difference in thigh-trunk angle from neutral to flexion. Clinical hip extension, or the change in thigh-trunk angle extension, was calculated as the difference in thigh-trunk angle from neutral to extension. The difference in LSS-LA from neutral to flexion (the change in LSS-LA flexion) and from neutral to extension (the change in LSS-LA extension) was also calculated. Finally, the change in SP flexion was calculated as the difference in SP from neutral to flexion. The change in SP extension was the difference in SP from neutral to extension.
“True hip joint flexion,” which reflects net motion occurring at the hip joint, was extrapolated from the X-rays as follows:
True Hip Joint Flexion = [ΔThigh-trunk Angle Flexion] – [ΔLSS-LA Flexion + ΔSP Flexion]
Similarly, “true hip joint extension,” which reflects net motion occurring at the hip joint, was calculated as follows:
True Hip Joint Extension = [ΔThigh-trunk Angle Extension] – [ΔLSS-LA Extension + ΔSP Extension] (Figure 2).
An orthopaedic surgery fellow performed all radiographic measurements on 3 separate occasions. The average of each measurement and final functional scores were plotted on an Excel worksheet (Microsoft; Redmond, WA, USA).
Statistical Analysis
Fisher’s exact test was used for the gender categorical variable between study and control groups. Due to the small sample size, the nonparametric Wilcoxin rank sum test was used to determine differences between study and control groups in the noncategorical (continuous) variables which included age, BMI, and follow-up months after surgery. Next, statistical analysis was performed on postoperative HHS, Oxford, and WOMAC scores as well as all radiographic measurements to detect differences in thigh-trunk and true hip joint ROM between DM-THA and 36-THA in flexion and extension. Finally, analysis was performed on the same radiographic parameters to detect the difference in ROM between THA-PL and THA-AL patients. Significance was set at p<0.05. All analyses were performed using SPSS software (SPSS Inc.; Chicago, IL, now called IBM SPSS). RESULTS
Demographics
There was no statistically significant difference between DM-THA and 36-THA in each of the matched demographical variables (Table 1). The mean age for the DM-THA was 60.90±3.83 years versus 66.2±8.65 years for the 36-THA group (p=0.110). In the DM-THA group, there were 10 males and 6 females versus 12 males and 8 females in the 36-THA group (p=1.000). BMI for DM-THA was 33.14±10.76 versus 31.41±7.10 in 36-THA (p=0.566). Follow-up time point since surgery was 19.61±4.78 months in DM-THA versus 18.13±3.14 months in 36-THA (p=0.276).
True Hip Joint Flexion = [ΔThigh-trunk Angle Flexion] – [ΔLSS-LA Flexion + ΔSP Flexion]
Similarly, “true hip joint extension,” which reflects net motion occurring at the hip joint, was calculated as follows:
True Hip Joint Extension = [ΔThigh-trunk Angle Extension] – [ΔLSS-LA Extension + ΔSP Extension] (Figure 2).
An orthopaedic surgery fellow performed all radiographic measurements on 3 separate occasions. The average of each measurement and final functional scores were plotted on an Excel worksheet (Microsoft; Redmond, WA, USA).
Statistical Analysis
Fisher’s exact test was used for the gender categorical variable between study and control groups. Due to the small sample size, the nonparametric Wilcoxin rank sum test was used to determine differences between study and control groups in the noncategorical (continuous) variables which included age, BMI, and follow-up months after surgery. Next, statistical analysis was performed on postoperative HHS, Oxford, and WOMAC scores as well as all radiographic measurements to detect differences in thigh-trunk and true hip joint ROM between DM-THA and 36-THA in flexion and extension. Finally, analysis was performed on the same radiographic parameters to detect the difference in ROM between THA-PL and THA-AL patients. Significance was set at p<0.05. All analyses were performed using SPSS software (SPSS Inc.; Chicago, IL, now called IBM SPSS). RESULTS
Demographics
There was no statistically significant difference between DM-THA and 36-THA in each of the matched demographical variables (Table 1). The mean age for the DM-THA was 60.90±3.83 years versus 66.2±8.65 years for the 36-THA group (p=0.110). In the DM-THA group, there were 10 males and 6 females versus 12 males and 8 females in the 36-THA group (p=1.000). BMI for DM-THA was 33.14±10.76 versus 31.41±7.10 in 36-THA (p=0.566). Follow-up time point since surgery was 19.61±4.78 months in DM-THA versus 18.13±3.14 months in 36-THA (p=0.276).

Functional Scores
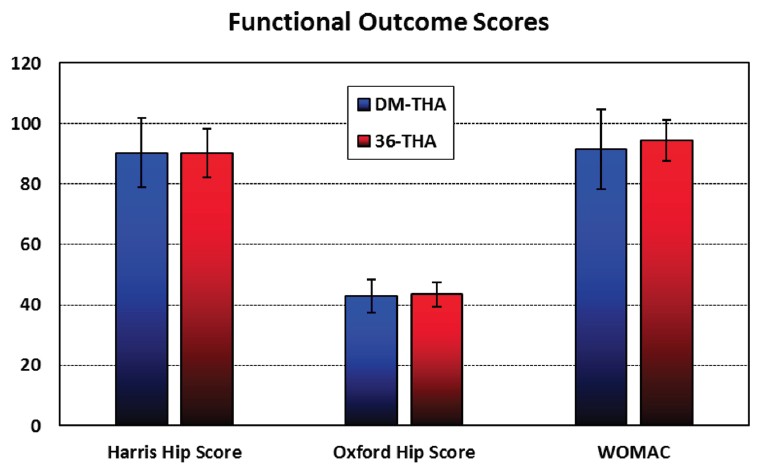
In DM-THA versus 36-THA, there was no statistically significant difference in HHS score (90.26±11.39 versus 90.27±7.98) (p=0.998), Oxford hip score (42.87±5.49 versus 43.47±4.09) (p=0.709), and WOMAC score (91.35±13.20 versus 94.43±6.78) (p=0.371) at the previously reported mean follow-up time (Figure 3).
Functional Scores
Effect of Head Size (DM-THA versus 36-THA)
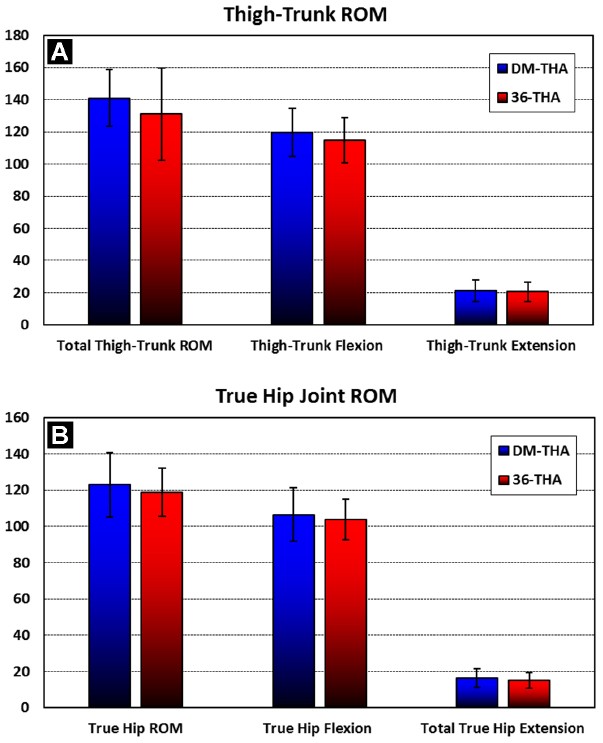
In DM-THA versus 36-THA, thigh-trunk flexion (119.67°±15.06° versus 114.74°±14.21°), thigh-trunk extension (21.27°±6.77° versus 20.47°±6.16°), and total thigh-trunk ROM (140.93°±17.51° versus 131.00°±28.81°) revealed no statistically significant difference between groups (p=0.199, 0.713 and 0.235, respectively) (Figure 4A). Similarly, true hip joint flexion (106.60°±14.98° versus 103.79°±11.31°), extension (16.33±5.07° versus 15.11±4.20°), and total true hip joint ROM (122.93°±17.66° versus 118.89°±13.23°) did not show a statistically significant difference between groups (p=0.525, 0.435, and 0.438, respectively) (Figure 4B).
Additionally, in DM-THA versus 36-THA, LSS flexion (11.87°±6.23° versus 9.26°±7.77°), extension (4.00°±3.12° versus 4.42°±4.51°), and total LSS ROM (15.87°±7.56° versus 13.58°±9.70°) did not show a significant difference between groups (p=0.283, 0.754, and, 0.444, respectively). Similarly, SP flexion (1.20°±1.01° versus 1.68°±1.00°), extension (0.93°±0.88° versus 0.95°±1.08°), and total SP ROM (2.13°±1.25° versus 2.63°±1.50°) did not show a significant difference between groups (p=0.163, 0.953, and 0.293, respectively).
Figure 5. Scatter plot showing relation between LSS pathology and thigh-trunk ROM. Patients with degenerative/stiff LSS (n=21) exhibited significantly less thigh-trunk flexion (mean 111.50°±13.99°) than patients with normal/flexible LSS (n=15) (124.64°±11.98°).
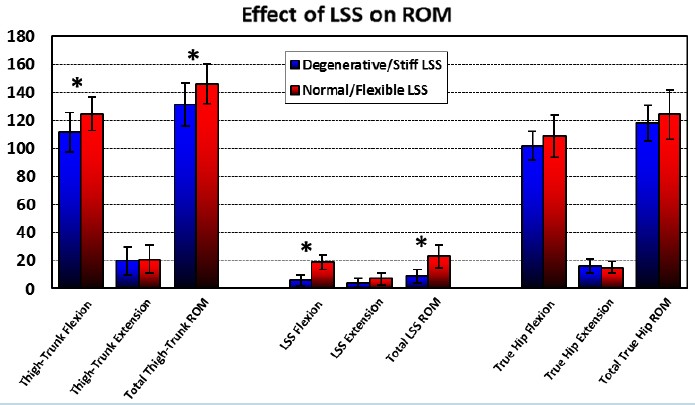
There was no correlation between gender and true hip ROM. Males and females showed no significant differences in true hip flexion, extension, and total true hip ROM in both DM-THA and 36-THA groups (p>0.05). However, there was a correlation between the degenerative condition and stiffness of the LSS and thigh-trunk ROM. The total LSS ROM in the study and control groups ranged from 0°-30° (median=15°). Patients with degenerative or stiff LSS as evidenced by radiological signs of lumbosacral spondylosis or fusion and/or diminished radiographic total LSS ROM (<15°) (n=21 patients) exhibited a statistically significant difference in thigh-trunk flexion (111.50°±13.99°). Thus, these patients also exhibited a significant difference in total thigh-trunk ROM (131.60°±15.39°) compared to patients who had radiological flexibility in their LSS segments (ROM>15°) without any signs of degenerative spine disease (n=15) and in whom thigh-trunk flexion was 124.64°±11.98° (p= 0.0053) and total thigh-trunk ROM was 146.14°±14.28° (p=0.006) (Figure 5). However, when comparing the group with LSS pathology/stiffness to that of normal LSS motion, true hip joint flexion (102.00°±10.28° versus 108.87°±15.14°), true hip joint extension (15.95°±5.10° versus 15.27°±3.94°), and total true hip ROM (117.95°±12.93° versus 124.13°±17.57°) showed no statistically significant difference (p=0.118, 0.664, and 0.232, respectively). Effect of Surgical Approach (THA-PL vs THA-AL)
There was no statistically significant difference in ROM between THA performed through a PL approach (n=18) and THA performed through a modified AL approach (n=18). In the THA-PL versus THA-AL group, true hip joint flexion (105.65°±10.06° versus 104.41°±15.56°), extension (16.00°±3.71° versus 15.29°±5.39°) and total true hip ROM (121.65°±11.16° versus 119.71°±18.76°) demonstrated no significant difference (p=0.778, 0.648, and 0.709, respectively) (Figure 6).
Functional Scores
Effect of Head Size (DM-THA versus 36-THA)
In DM-THA versus 36-THA, thigh-trunk flexion (119.67°±15.06° versus 114.74°±14.21°), thigh-trunk extension (21.27°±6.77° versus 20.47°±6.16°), and total thigh-trunk ROM (140.93°±17.51° versus 131.00°±28.81°) revealed no statistically significant difference between groups (p=0.199, 0.713 and 0.235, respectively) (Figure 4A). Similarly, true hip joint flexion (106.60°±14.98° versus 103.79°±11.31°), extension (16.33±5.07° versus 15.11±4.20°), and total true hip joint ROM (122.93°±17.66° versus 118.89°±13.23°) did not show a statistically significant difference between groups (p=0.525, 0.435, and 0.438, respectively) (Figure 4B).
Additionally, in DM-THA versus 36-THA, LSS flexion (11.87°±6.23° versus 9.26°±7.77°), extension (4.00°±3.12° versus 4.42°±4.51°), and total LSS ROM (15.87°±7.56° versus 13.58°±9.70°) did not show a significant difference between groups (p=0.283, 0.754, and, 0.444, respectively). Similarly, SP flexion (1.20°±1.01° versus 1.68°±1.00°), extension (0.93°±0.88° versus 0.95°±1.08°), and total SP ROM (2.13°±1.25° versus 2.63°±1.50°) did not show a significant difference between groups (p=0.163, 0.953, and 0.293, respectively).
Figure 5. Scatter plot showing relation between LSS pathology and thigh-trunk ROM. Patients with degenerative/stiff LSS (n=21) exhibited significantly less thigh-trunk flexion (mean 111.50°±13.99°) than patients with normal/flexible LSS (n=15) (124.64°±11.98°).
There was no correlation between gender and true hip ROM. Males and females showed no significant differences in true hip flexion, extension, and total true hip ROM in both DM-THA and 36-THA groups (p>0.05). However, there was a correlation between the degenerative condition and stiffness of the LSS and thigh-trunk ROM. The total LSS ROM in the study and control groups ranged from 0°-30° (median=15°). Patients with degenerative or stiff LSS as evidenced by radiological signs of lumbosacral spondylosis or fusion and/or diminished radiographic total LSS ROM (<15°) (n=21 patients) exhibited a statistically significant difference in thigh-trunk flexion (111.50°±13.99°). Thus, these patients also exhibited a significant difference in total thigh-trunk ROM (131.60°±15.39°) compared to patients who had radiological flexibility in their LSS segments (ROM>15°) without any signs of degenerative spine disease (n=15) and in whom thigh-trunk flexion was 124.64°±11.98° (p= 0.0053) and total thigh-trunk ROM was 146.14°±14.28° (p=0.006) (Figure 5). However, when comparing the group with LSS pathology/stiffness to that of normal LSS motion, true hip joint flexion (102.00°±10.28° versus 108.87°±15.14°), true hip joint extension (15.95°±5.10° versus 15.27°±3.94°), and total true hip ROM (117.95°±12.93° versus 124.13°±17.57°) showed no statistically significant difference (p=0.118, 0.664, and 0.232, respectively). Effect of Surgical Approach (THA-PL vs THA-AL)
There was no statistically significant difference in ROM between THA performed through a PL approach (n=18) and THA performed through a modified AL approach (n=18). In the THA-PL versus THA-AL group, true hip joint flexion (105.65°±10.06° versus 104.41°±15.56°), extension (16.00°±3.71° versus 15.29°±5.39°) and total true hip ROM (121.65°±11.16° versus 119.71°±18.76°) demonstrated no significant difference (p=0.778, 0.648, and 0.709, respectively) (Figure 6).

DISCUSSION
The large diameter effective head concept of DM-THA allows an increase in the head-neck ratio. This effective head concept has the theoretical advantage of increasing ROM to impingement and jump distance required for dislocation, therefore increasing stability [3-8,10-16]. Large diameter (≥36 mm) conventional THA has evolved from the same concept of increasing head-neck ratio to increase stability, which became popular after successful reduction in dislocation rates [17-20]. Because there is limited basic science on hip ROM after DM-THA compared to 36-THA, the investigators were particularly interested in hip ROM with a dual mobility design [4-8,10-16].
There were limitations to this nonrandomized study. The number of patients in each group was small as they were the only patients willing to volunteer. However, both study and control groups were matched in terms of age, sex, and BMI, which might reduce such selection bias. There were no radiographic measurements performed on the contralateral, nonoperated hip, which could have served as an internal control. Concerns with overexposure to high doses of ionizing radiation and justification of such a procedure would have made implementing this protocol extremely difficult.
A single orthopaedic surgeon performed all radiographic measurements, which may infer observer bias. However, most radiographic landmarks and measurements in this study were well established in literature with excellent intraobserver and interobserver reliability. Additionally, all measurements were taken on 3 separate occasions, and values were averaged to eliminate intraobserver reliability redundancies. Finally, several factors were identified in determining in vivo ROM after THA, including prosthetic cup abduction and anteversion, as well as femoral neck anteversion. These factors could have introduced confounding variables to THA ROM but were minimized as a single surgeon case series and a consistency in operative technique [31].
In vivo ROM data in this study agree with computer simulations and in vitro studies [21,22,32]. While these studies may demonstrate high ROM prior to impingement once the soft tissues are considered, Incavo et al. demonstrated that hip flexion was limited to 125° on average in a cadaver model [32]. In a recent 3D computer-simulated study based on human cadaver hips, Klingenstein et al. found no statistically significant difference in the mean range of motion during straight flexion and extension between the dual mobility cup, 36 mm head THA, and 28 mm head THA [33]. Similar results were found when comparing unipolar versus bipolar hip prosthesis [34]. While no effect of gender on ROM was found with either prosthesis, the spinal degeneration and stiffness on the clinical hip ROM (thigh-trunk motion) without affecting true hip ROM was of interest. Imaging of THA patients may underestimate the analysis of the suprapelvic motion segment, a crucial part of the sagittal balance of the trunk. Spino-pelvic position and motion are complex and show wide variations [35,36].
The main aim of this study was to analyze true hip ROM in DM-THA versus 36-THA. Analysis of spinal pathology was not scrutinized in the construction of the study and control groups, which might introduce confounding variables. In this study, LSS ROM did not show significant differences between DM-THA and 36-THA groups, which could imply equal distribution of spinal pathology among matched groups. The findings, though pertinent to LSS degenerative condition and contribution to motion, warrant further investigations focusing on the role of spino-pelvic biomechanics and its repercussions on postoperative THA ROM.
The effect of surgical approach on postoperative ROM remains under investigated. While some studies have found that surgical approach has no effect on postoperative gait mechanics after THA, there are limited reports on THA postoperative ROM via different surgical approaches [23,25,27]. This study demonstrates no significant difference in hip flexion or extension between THA patients operated on via a PL approach as opposed to those who had a modified AL approach.
Finally, the current study demonstrated absence of superiority in activity levels between the study and control groups. This finding was evident by absence of any statistically significant difference in HHS, Oxford, and WOMAC scores between DM-THA and 36-THA (p>0.05). These fi- ndings are in agreement with the study by Allen et al., which showed that while comparing 3 groups of THAs (<36 mm head, 36 mm head, >36 mm head), increasing the size of the femoral head did not significantly improve the functional outcome at 1 year. Yet the use of a 36 mm or greater femoral head did lower the dislocation rate [37]. Another recent study confirmed the aforementioned findings, where Epinette et al. showed no significant difference between DM-THA and 36-THA groups in terms of pain, range of motion, or functional score [38]. CONCLUSIONS
DM-THA does not provide superior ROM or functional outcomes compared to 36-THA, as evidenced by digital radiography and clinical hip scores. PL versus modified AL surgical approach, with presumptive violation of hip extensors or flexors, does not affect postoperative hip extension or flexion. THA patients with a flexible LSS may exhibit apparent increased clinical hip ROM due to compensatory movement at the LSS rather than actual increase in true hip ROM. REFERENCES
[1] Farizon F, de Lavison R, Azoulai JJ, Bousquet G. Results with a cementless alumina-coated cup with dual mobility. A twelve-year follow-up study. Int Orthop. 1998;22(4):219-24.
[2] Langlais FL, Ropars M, Gaucher F, et al. Dual mobility cemented cups have low dislocation rates in THA revisions. Clin Orthop Relat Res. 2008;466(2):389-95.
[3] Philippot R, Adam P, Reckhaus M, et al. Prevention of dislocation in total hip revision surgery using a dual mobility design. Orthop Traumatol Surg Res. 2009;95(6):407-13.
[4] Guyen O, Pibarot V, Vaz G, et al. Unconstrained tripolar implants for primary total hip arthroplasty in patients at risk for dislocation. J Arthroplasty. 2007;22(6):849-58.
[5] Philippot R, Camilleri JP, Boyer B, et al. The use of a dual-articulation acetabular cup system to prevent dislocation after primary total hip arthroplasty: analysis of 384 cases at a mean follow-up of 15 years. Int Orthop. 2009;33(4):927-32.
[6] Tarasevicius S, Busevicius M, Robertssson O, Wingstrand H. Dual mobility cup reduces dislocation rate after arthroplasty for femoral neck fracture. BMC Musculoskelet Disord. 2010;11:175.
[7] Vielpeau C, Lebel B, Ardouin L, et al. The dual mobility socket concept: experience with 668 cases. Int Orthop. 2011;35(2):225-30.
[8] Bouchet R, Mercier N, Saragaglia D. Posterior approach and dislocation rate: a 213 total hip replacements case-control study comparing the dual mobility cup with a conventional 28-mm metal head/polyethylene prosthesis. Orthop Traumatol Surg Res. 2011;97(1):2-7.
[9] Hailer NP, Weiss RJ, Stark A, Karrholm J. The risk of revision due to dislocation after total hip arthroplasty depends on surgical approach, femoral head size, sex, and primary diagnosis. An analysis of 78,098 operations in the Swedish Hip Arthroplasty Register. Acta Orthop. 2012;83(5):442-8.
[10] Boyer B, Philippot R, Gerringer J, Farizon F. Primary total hip arthroplasty with dual mobility socket to prevent dislocation: a 22-year follow-up of 240 hips. Int Orthop. 2012;36(3):511-8.
[11] Hamadouche M, Arnould H, Bouxin B. Is a cementless dual mobility socket in primary THA a reasonable option? Clin Orthop Relat Res. 2012;470(11):3048-53.
[12] Combes A, Migaud H, Girard J, et al. Low rate of dislocation of dual-mobility cups in primary total hip arthroplasty. Clin Orthop Relat Res. 2013; 471(12):3891-900.
[13] Guyen O, Pibarot V, Vaz G. Use of a dual mobility socket to manage total hip arthroplasty instability. Clin Orthop Relat Res. 2009;467(2):465-72.
[14] Hamadouche M, Biau DJ, Huten D, et al. The use of a cemented dual mobility socket to treat recurrent dislocation. Clin Orthop Relat Res. 2010;468(12):3248-54.
[15] Leiber-Wackenheim F, Brunschweiler B, Ehlinger M. Treatment of recurrent THR dislocation using of a cementless dual-mobility cup: a 59 cases series with a mean 8 years’ follow-up. Orthop Traumatol Surg Res. 2011;97(1):8-13.
[16] Hailer NP, Weiss RJ, Stark A, Karrholm J. Dual-mobility cups for revision due to instability are associated with a low rate of re-revisions due to dislocation: 228 patients from the Swedish Hip Arthroplasty Register. Acta Orthop. 2012;83(6):566-71.
[17] Stroh DA, Issa K, Johnson AJ, et al. Reduced dislocation rates and excellent functional outcomes with large-diameter femoral heads. J Arthroplasty. 2013;28(8):1415-20.
[18] Plate JF, Seyler TM, Stroh DA, et al. Risk of dislocation using large- vs. small-diameter femoral heads in total hip arthroplasty. BMC Res Notes. 2012;5:553.
[19] Howie DW, Holubowycz OT, Middleton R, Large Articulation Study Group. Large femoral heads decrease the incidence of dislocation after total hip arthroplasty: a randomized controlled trial. J Bone Joint Surg Am. 2012;94(12):1095-102.
[20] Lombardi AV Jr., Skeels MD, Berend KR, et al. Do large heads enhance stability and restore native anatomy in primary total hip arthroplasty? Clin Orthop Relat Res. 2011;469(6):1547-53.
[21] Klingenstein GG, Yeager AM, Lipman JD, Westrich GH. Computerized range of motion analysis following dual mobility total hip arthroplasty, traditional total hip arthroplasty, and hip resurfacing. J Arthroplasty. 2013;28(7):1173-6.
[22] Burroughs BR, Hallstrom B, Golladay GJ, et al. Range of motion and stability in total hip arthroplasty with 28-, 32-, 38-, and 44-mm femoral head sizes. J Arthroplasty. 2005;20(1):11-9.
[23] Queen RM, Butler RJ, Watters TS, et al. The effect of total hip arthroplasty surgical approach on postoperative gait mechanics. J Arthroplasty. 2011;26(6 Suppl):66-71.
[24] Varin D, Lamontagne M, Beaule PE. Does the anterior approach for THA provide closer-to-normal lower-limb motion? J Arthroplasty. 2013;28(8):1401-7.
[25] Madsen MS, Ritter MA, Morris HH, et al. The effect of total hip arthroplasty surgical approach on gait. J Orthop Res. 2004;22(1):44-50.
[26] Jolles BM, Bogoch ER. Surgical approach for total hip arthroplasty: direct lateral or posterior? J Rheumatol. 2004;31(9):1790-6.
[27] Jolles BM, Bogoch ER. Posterior versus lateral surgical approach for total hip arthroplasty in adults with osteoarthritis. Cochrane Database Syst Rev. 2006;(3):CD003828.
[28] Lazennec JY, Charlot N, Gorin N, et al. Hip-spine relationship: a radio-anatomical study for optimization in acetabular cup positioning. Surg Radiol Anat. 2004;26(2):136-44.
[29] Roussouly P, Gollogly S, Berthonnaud E, Dimnet J. Classification of the normal variation in the sagittal alignment of the human lumbar spine and pelvis in the standing position. Spine (Phila Pa 1976). 2005;30(3):346-53.
[30] Lewinnek GE, Lewis JL, Tarr R, et al. Dislocations after total hip-replacement arthroplasties. J Bone Joint Surg Am. 1978;60(2):217-20.
[31] Yoshimine F, Ginbayashi K. A mathematical formula to calculate the theoretical range of motion for total hip replacement. J Biomech. 2002;35(7):989-93.
[32] Incavo SJ, Thompson MT, Gold JE, et al. Which procedure better restores intact hip range of motion: total hip arthroplasty or resurfacing? A combined cadaveric and computer simulation study. J Arthroplasty. 2011;26(3):391-7.
[33] Klingenstein GG, Yeager AM, Lipman JD, Westrich GH. Computerized range of motion analysis following dual mobility total hip arthroplasty, traditional total hip arthroplasty, and hip resurfacing. J Arthroplasty. 2013;28(7):1173-6.
[34] Jia Z, Dinq F, Wu Y, et al. Unipolar versus bipolar hemiarthroplasty for displaced femoral neck fractures: a systematic review and meta-analysis of randomized controlled trials. J Orthop Surg Res. 2015.10:8.
[35] Babisch JW, Layher F, Amiot LP. The rationale for tilt-adjusted acetabular cup navigation. J Bone Joint Surg Am. 2008;90(2):357-65.
[36] DiGioia AM, Hafez MA, Jaramaz B, et al. Functional pelvic orientation measured from lateral standing and sitting radiographs. Clin Orthop Relat Res. 2006;453:272-6.
[37] Allen CL, Hooper GJ, Frampton CM. Do larger femoral heads improve the functional outcome in total hip arthroplasty? J Arthroplasty. 2014;29(2):401-4.
[38] Epinette JA. Clinical outcomes, survivorship and adverse events with mobile-bearings versus fixed-bearings in hip arthroplasty-a prospective comparative cohort study of 143 ADM versus 130 trident cups at 2 to 6-year follow-up. J Arthroplasty. 2015;30(2):241-8.
The large diameter effective head concept of DM-THA allows an increase in the head-neck ratio. This effective head concept has the theoretical advantage of increasing ROM to impingement and jump distance required for dislocation, therefore increasing stability [3-8,10-16]. Large diameter (≥36 mm) conventional THA has evolved from the same concept of increasing head-neck ratio to increase stability, which became popular after successful reduction in dislocation rates [17-20]. Because there is limited basic science on hip ROM after DM-THA compared to 36-THA, the investigators were particularly interested in hip ROM with a dual mobility design [4-8,10-16].
There were limitations to this nonrandomized study. The number of patients in each group was small as they were the only patients willing to volunteer. However, both study and control groups were matched in terms of age, sex, and BMI, which might reduce such selection bias. There were no radiographic measurements performed on the contralateral, nonoperated hip, which could have served as an internal control. Concerns with overexposure to high doses of ionizing radiation and justification of such a procedure would have made implementing this protocol extremely difficult.
A single orthopaedic surgeon performed all radiographic measurements, which may infer observer bias. However, most radiographic landmarks and measurements in this study were well established in literature with excellent intraobserver and interobserver reliability. Additionally, all measurements were taken on 3 separate occasions, and values were averaged to eliminate intraobserver reliability redundancies. Finally, several factors were identified in determining in vivo ROM after THA, including prosthetic cup abduction and anteversion, as well as femoral neck anteversion. These factors could have introduced confounding variables to THA ROM but were minimized as a single surgeon case series and a consistency in operative technique [31].
In vivo ROM data in this study agree with computer simulations and in vitro studies [21,22,32]. While these studies may demonstrate high ROM prior to impingement once the soft tissues are considered, Incavo et al. demonstrated that hip flexion was limited to 125° on average in a cadaver model [32]. In a recent 3D computer-simulated study based on human cadaver hips, Klingenstein et al. found no statistically significant difference in the mean range of motion during straight flexion and extension between the dual mobility cup, 36 mm head THA, and 28 mm head THA [33]. Similar results were found when comparing unipolar versus bipolar hip prosthesis [34]. While no effect of gender on ROM was found with either prosthesis, the spinal degeneration and stiffness on the clinical hip ROM (thigh-trunk motion) without affecting true hip ROM was of interest. Imaging of THA patients may underestimate the analysis of the suprapelvic motion segment, a crucial part of the sagittal balance of the trunk. Spino-pelvic position and motion are complex and show wide variations [35,36].
The main aim of this study was to analyze true hip ROM in DM-THA versus 36-THA. Analysis of spinal pathology was not scrutinized in the construction of the study and control groups, which might introduce confounding variables. In this study, LSS ROM did not show significant differences between DM-THA and 36-THA groups, which could imply equal distribution of spinal pathology among matched groups. The findings, though pertinent to LSS degenerative condition and contribution to motion, warrant further investigations focusing on the role of spino-pelvic biomechanics and its repercussions on postoperative THA ROM.
The effect of surgical approach on postoperative ROM remains under investigated. While some studies have found that surgical approach has no effect on postoperative gait mechanics after THA, there are limited reports on THA postoperative ROM via different surgical approaches [23,25,27]. This study demonstrates no significant difference in hip flexion or extension between THA patients operated on via a PL approach as opposed to those who had a modified AL approach.
Finally, the current study demonstrated absence of superiority in activity levels between the study and control groups. This finding was evident by absence of any statistically significant difference in HHS, Oxford, and WOMAC scores between DM-THA and 36-THA (p>0.05). These fi- ndings are in agreement with the study by Allen et al., which showed that while comparing 3 groups of THAs (<36 mm head, 36 mm head, >36 mm head), increasing the size of the femoral head did not significantly improve the functional outcome at 1 year. Yet the use of a 36 mm or greater femoral head did lower the dislocation rate [37]. Another recent study confirmed the aforementioned findings, where Epinette et al. showed no significant difference between DM-THA and 36-THA groups in terms of pain, range of motion, or functional score [38]. CONCLUSIONS
DM-THA does not provide superior ROM or functional outcomes compared to 36-THA, as evidenced by digital radiography and clinical hip scores. PL versus modified AL surgical approach, with presumptive violation of hip extensors or flexors, does not affect postoperative hip extension or flexion. THA patients with a flexible LSS may exhibit apparent increased clinical hip ROM due to compensatory movement at the LSS rather than actual increase in true hip ROM. REFERENCES
[1] Farizon F, de Lavison R, Azoulai JJ, Bousquet G. Results with a cementless alumina-coated cup with dual mobility. A twelve-year follow-up study. Int Orthop. 1998;22(4):219-24.
[2] Langlais FL, Ropars M, Gaucher F, et al. Dual mobility cemented cups have low dislocation rates in THA revisions. Clin Orthop Relat Res. 2008;466(2):389-95.
[3] Philippot R, Adam P, Reckhaus M, et al. Prevention of dislocation in total hip revision surgery using a dual mobility design. Orthop Traumatol Surg Res. 2009;95(6):407-13.
[4] Guyen O, Pibarot V, Vaz G, et al. Unconstrained tripolar implants for primary total hip arthroplasty in patients at risk for dislocation. J Arthroplasty. 2007;22(6):849-58.
[5] Philippot R, Camilleri JP, Boyer B, et al. The use of a dual-articulation acetabular cup system to prevent dislocation after primary total hip arthroplasty: analysis of 384 cases at a mean follow-up of 15 years. Int Orthop. 2009;33(4):927-32.
[6] Tarasevicius S, Busevicius M, Robertssson O, Wingstrand H. Dual mobility cup reduces dislocation rate after arthroplasty for femoral neck fracture. BMC Musculoskelet Disord. 2010;11:175.
[7] Vielpeau C, Lebel B, Ardouin L, et al. The dual mobility socket concept: experience with 668 cases. Int Orthop. 2011;35(2):225-30.
[8] Bouchet R, Mercier N, Saragaglia D. Posterior approach and dislocation rate: a 213 total hip replacements case-control study comparing the dual mobility cup with a conventional 28-mm metal head/polyethylene prosthesis. Orthop Traumatol Surg Res. 2011;97(1):2-7.
[9] Hailer NP, Weiss RJ, Stark A, Karrholm J. The risk of revision due to dislocation after total hip arthroplasty depends on surgical approach, femoral head size, sex, and primary diagnosis. An analysis of 78,098 operations in the Swedish Hip Arthroplasty Register. Acta Orthop. 2012;83(5):442-8.
[10] Boyer B, Philippot R, Gerringer J, Farizon F. Primary total hip arthroplasty with dual mobility socket to prevent dislocation: a 22-year follow-up of 240 hips. Int Orthop. 2012;36(3):511-8.
[11] Hamadouche M, Arnould H, Bouxin B. Is a cementless dual mobility socket in primary THA a reasonable option? Clin Orthop Relat Res. 2012;470(11):3048-53.
[12] Combes A, Migaud H, Girard J, et al. Low rate of dislocation of dual-mobility cups in primary total hip arthroplasty. Clin Orthop Relat Res. 2013; 471(12):3891-900.
[13] Guyen O, Pibarot V, Vaz G. Use of a dual mobility socket to manage total hip arthroplasty instability. Clin Orthop Relat Res. 2009;467(2):465-72.
[14] Hamadouche M, Biau DJ, Huten D, et al. The use of a cemented dual mobility socket to treat recurrent dislocation. Clin Orthop Relat Res. 2010;468(12):3248-54.
[15] Leiber-Wackenheim F, Brunschweiler B, Ehlinger M. Treatment of recurrent THR dislocation using of a cementless dual-mobility cup: a 59 cases series with a mean 8 years’ follow-up. Orthop Traumatol Surg Res. 2011;97(1):8-13.
[16] Hailer NP, Weiss RJ, Stark A, Karrholm J. Dual-mobility cups for revision due to instability are associated with a low rate of re-revisions due to dislocation: 228 patients from the Swedish Hip Arthroplasty Register. Acta Orthop. 2012;83(6):566-71.
[17] Stroh DA, Issa K, Johnson AJ, et al. Reduced dislocation rates and excellent functional outcomes with large-diameter femoral heads. J Arthroplasty. 2013;28(8):1415-20.
[18] Plate JF, Seyler TM, Stroh DA, et al. Risk of dislocation using large- vs. small-diameter femoral heads in total hip arthroplasty. BMC Res Notes. 2012;5:553.
[19] Howie DW, Holubowycz OT, Middleton R, Large Articulation Study Group. Large femoral heads decrease the incidence of dislocation after total hip arthroplasty: a randomized controlled trial. J Bone Joint Surg Am. 2012;94(12):1095-102.
[20] Lombardi AV Jr., Skeels MD, Berend KR, et al. Do large heads enhance stability and restore native anatomy in primary total hip arthroplasty? Clin Orthop Relat Res. 2011;469(6):1547-53.
[21] Klingenstein GG, Yeager AM, Lipman JD, Westrich GH. Computerized range of motion analysis following dual mobility total hip arthroplasty, traditional total hip arthroplasty, and hip resurfacing. J Arthroplasty. 2013;28(7):1173-6.
[22] Burroughs BR, Hallstrom B, Golladay GJ, et al. Range of motion and stability in total hip arthroplasty with 28-, 32-, 38-, and 44-mm femoral head sizes. J Arthroplasty. 2005;20(1):11-9.
[23] Queen RM, Butler RJ, Watters TS, et al. The effect of total hip arthroplasty surgical approach on postoperative gait mechanics. J Arthroplasty. 2011;26(6 Suppl):66-71.
[24] Varin D, Lamontagne M, Beaule PE. Does the anterior approach for THA provide closer-to-normal lower-limb motion? J Arthroplasty. 2013;28(8):1401-7.
[25] Madsen MS, Ritter MA, Morris HH, et al. The effect of total hip arthroplasty surgical approach on gait. J Orthop Res. 2004;22(1):44-50.
[26] Jolles BM, Bogoch ER. Surgical approach for total hip arthroplasty: direct lateral or posterior? J Rheumatol. 2004;31(9):1790-6.
[27] Jolles BM, Bogoch ER. Posterior versus lateral surgical approach for total hip arthroplasty in adults with osteoarthritis. Cochrane Database Syst Rev. 2006;(3):CD003828.
[28] Lazennec JY, Charlot N, Gorin N, et al. Hip-spine relationship: a radio-anatomical study for optimization in acetabular cup positioning. Surg Radiol Anat. 2004;26(2):136-44.
[29] Roussouly P, Gollogly S, Berthonnaud E, Dimnet J. Classification of the normal variation in the sagittal alignment of the human lumbar spine and pelvis in the standing position. Spine (Phila Pa 1976). 2005;30(3):346-53.
[30] Lewinnek GE, Lewis JL, Tarr R, et al. Dislocations after total hip-replacement arthroplasties. J Bone Joint Surg Am. 1978;60(2):217-20.
[31] Yoshimine F, Ginbayashi K. A mathematical formula to calculate the theoretical range of motion for total hip replacement. J Biomech. 2002;35(7):989-93.
[32] Incavo SJ, Thompson MT, Gold JE, et al. Which procedure better restores intact hip range of motion: total hip arthroplasty or resurfacing? A combined cadaveric and computer simulation study. J Arthroplasty. 2011;26(3):391-7.
[33] Klingenstein GG, Yeager AM, Lipman JD, Westrich GH. Computerized range of motion analysis following dual mobility total hip arthroplasty, traditional total hip arthroplasty, and hip resurfacing. J Arthroplasty. 2013;28(7):1173-6.
[34] Jia Z, Dinq F, Wu Y, et al. Unipolar versus bipolar hemiarthroplasty for displaced femoral neck fractures: a systematic review and meta-analysis of randomized controlled trials. J Orthop Surg Res. 2015.10:8.
[35] Babisch JW, Layher F, Amiot LP. The rationale for tilt-adjusted acetabular cup navigation. J Bone Joint Surg Am. 2008;90(2):357-65.
[36] DiGioia AM, Hafez MA, Jaramaz B, et al. Functional pelvic orientation measured from lateral standing and sitting radiographs. Clin Orthop Relat Res. 2006;453:272-6.
[37] Allen CL, Hooper GJ, Frampton CM. Do larger femoral heads improve the functional outcome in total hip arthroplasty? J Arthroplasty. 2014;29(2):401-4.
[38] Epinette JA. Clinical outcomes, survivorship and adverse events with mobile-bearings versus fixed-bearings in hip arthroplasty-a prospective comparative cohort study of 143 ADM versus 130 trident cups at 2 to 6-year follow-up. J Arthroplasty. 2015;30(2):241-8.