
The Rate and Progression of Facet Arthrodesis after Transforaminal Lumbar Interbody Fusion
Christopher Chaput, MD; Shayan Vadie, BS, MS; Yolanda Munoz Maldonado, PhD
Department of Orthopaedic Surgery, Baylor Scott & White Health; Temple, TX, USA
Corresponding Author:Christopher Chaput, MD, Department of Orthopaedic Surgery, Baylor Scott & White Health, 2401 S. 31st St., Temple, TX 76508, USA; christopher.chaput@BSWHealth.org
DOI: 10.18600/toj.020103
INTRODUCTION
It remains unknown exactly how much facet decortication, articular preparation, and graft volume is required to reliably obtain facet arthrodesis in an open or minimally invasive setting. With formal preparation of the articular surface and use of autograft to pack the joint, healing rates of up to 92% have been documented [1]. However, some investigators have documented fusion at the facet with simple immobilization and compression across the articular surface, even in absence of decortication or grafting [2,3].
Traditionally, posterolateral lumbar fusion requires a fairly extensive dissection away from midline, often leading to detachment of multifidus origin or denervation of its fibers. The amount of retraction needed to perform a traditional open lumbar instrumentation and fusion can also lead to significant crush injury to the paraspinal musculature. This has been linked to an increase in postoperative pain, an increased risk of infection, and an increased risk of failed back surgery syndrome [4,5]. For these reasons—as well as patient demand—less invasive surgical (LIS) techniques have gained popularity in recent years, and the overall percentage of cases using these techniques is expected to continue to climb [6]. Understanding the rate and manner of facet fusion may be increasingly important as LIS procedures gain popularity, as some LIS procedures may make formal facet preparation and grafting difficult or impossible.
The primary aim of this study is to examine the rate and geographic progression of lumbar facet fusion in the setting of transforaminal lumbar interbody fusion (TLIF). The secondary aim of this study is to determine if there is a correlation between clinical outcomes and facet joint fusion. MATERIALS & METHODS
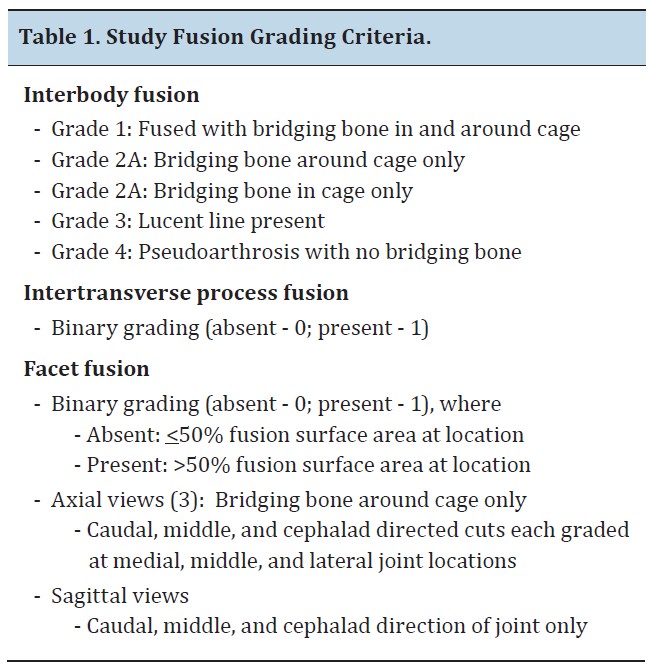
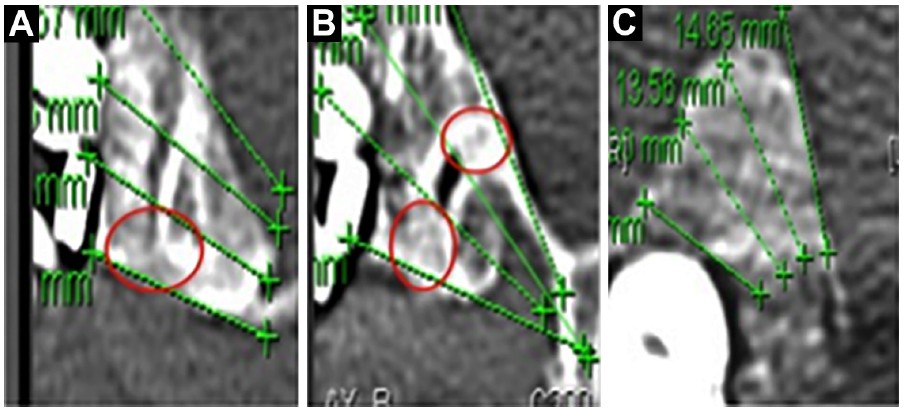
The study is a post hoc analysis of prospective clinical data and computed tomography (CT) scans obtained from 3 separate TLIF studies performed at a single institution. All patients enrolled in these studies were pooled; no patients were excluded. In total, 39 patients, 24 (61.5%) women and 15 (38.5%) men, with mean age of 57 years (standard deviation of 13.5), were enrolled at time of surgery. Primary diagnoses at time of surgery included degenerative spondylolisthesis, scoliosis, lumbar disc herniation, and lumbar stenosis. All TLIF procedures were carried out per standard protocol with an open posterolateral fusion performed with interbody placement [7]. The entire facet was removed on the approach side, and the contralateral facet was spared and minimally debrided with a Leksell rongeur in the context of standard intertransverse fusion. Pedicle screw instrumentation was used to compress across the cage, unless concerns about scoliosis correction dictated otherwise. Fusion was aided by packing the disc space, interbody cages, and intertranverse region with either Healos (DePuy Spine; Raynham, MA) soaked in bone marrow aspirate (19 patients) or iliac crest autograft (16 patients). One study involving 4 patients specified that no posterolateral or intertransverse preparation or grafting be performed. In these patients, only the interbody space was packed with graft. Based on original study protocols, approximately half the patients had 1-year and 2-year CT scans, and half had only 2-year CT scans available for review. If a patient had multiple fusions (treatment on more than 1 vertebra), 1 level was randomly chosen for inclusion in our study while the other levels were excluded. This was done so the statistical analysis could be performed on independent data and without bias. We developed a geographic grading system based on a scale from 0 (no evidence of bridging bone) to 9 (complete obliteration of facet joint space), and termed the patients' numerical score the total facet fusion score (TFFS). Using bone window with 2x magnification, 6 axial slices through each facet joint were displayed. A sagittal cut through the middle of the facet joint was then referenced to analyze the 6 axial cuts and select the 3 axial cuts that best represented the cephalad, middle, and caudal aspects of the facet joint. After the 3 best axial cuts were chosen to grade, each was divided into thirds to represent the lateral 1/3, middle 1/3, and medial 1/3 of the facet joint at that level. Each area was then given a binary score of 0 or 1. A 0 was given if less than 50% of that area was bridged with bone. A 1 was given if bridging bone covered more than 50% of that area. The maximum score for any given axial image was 3 (>50% bridging bone across lateral 1/3, middle 1/3, and medial 1/3 of joint). The scores from the 3 axial images were added to get the patients’ TFFS. A TFFS of 9 would imply all three axial images were scored a 3. We considered a TFFS of > 4 was definitely fused, 3 was probably fused, and those with score <3 were considered not fused. The CT scans at 1-year and 2-year follow up were then compared to examine the rate and geographic progression of fusion over time.
It remains unknown exactly how much facet decortication, articular preparation, and graft volume is required to reliably obtain facet arthrodesis in an open or minimally invasive setting. With formal preparation of the articular surface and use of autograft to pack the joint, healing rates of up to 92% have been documented [1]. However, some investigators have documented fusion at the facet with simple immobilization and compression across the articular surface, even in absence of decortication or grafting [2,3].
Traditionally, posterolateral lumbar fusion requires a fairly extensive dissection away from midline, often leading to detachment of multifidus origin or denervation of its fibers. The amount of retraction needed to perform a traditional open lumbar instrumentation and fusion can also lead to significant crush injury to the paraspinal musculature. This has been linked to an increase in postoperative pain, an increased risk of infection, and an increased risk of failed back surgery syndrome [4,5]. For these reasons—as well as patient demand—less invasive surgical (LIS) techniques have gained popularity in recent years, and the overall percentage of cases using these techniques is expected to continue to climb [6]. Understanding the rate and manner of facet fusion may be increasingly important as LIS procedures gain popularity, as some LIS procedures may make formal facet preparation and grafting difficult or impossible.
The primary aim of this study is to examine the rate and geographic progression of lumbar facet fusion in the setting of transforaminal lumbar interbody fusion (TLIF). The secondary aim of this study is to determine if there is a correlation between clinical outcomes and facet joint fusion. MATERIALS & METHODS
The study is a post hoc analysis of prospective clinical data and computed tomography (CT) scans obtained from 3 separate TLIF studies performed at a single institution. All patients enrolled in these studies were pooled; no patients were excluded. In total, 39 patients, 24 (61.5%) women and 15 (38.5%) men, with mean age of 57 years (standard deviation of 13.5), were enrolled at time of surgery. Primary diagnoses at time of surgery included degenerative spondylolisthesis, scoliosis, lumbar disc herniation, and lumbar stenosis. All TLIF procedures were carried out per standard protocol with an open posterolateral fusion performed with interbody placement [7]. The entire facet was removed on the approach side, and the contralateral facet was spared and minimally debrided with a Leksell rongeur in the context of standard intertransverse fusion. Pedicle screw instrumentation was used to compress across the cage, unless concerns about scoliosis correction dictated otherwise. Fusion was aided by packing the disc space, interbody cages, and intertranverse region with either Healos (DePuy Spine; Raynham, MA) soaked in bone marrow aspirate (19 patients) or iliac crest autograft (16 patients). One study involving 4 patients specified that no posterolateral or intertransverse preparation or grafting be performed. In these patients, only the interbody space was packed with graft. Based on original study protocols, approximately half the patients had 1-year and 2-year CT scans, and half had only 2-year CT scans available for review. If a patient had multiple fusions (treatment on more than 1 vertebra), 1 level was randomly chosen for inclusion in our study while the other levels were excluded. This was done so the statistical analysis could be performed on independent data and without bias. We developed a geographic grading system based on a scale from 0 (no evidence of bridging bone) to 9 (complete obliteration of facet joint space), and termed the patients' numerical score the total facet fusion score (TFFS). Using bone window with 2x magnification, 6 axial slices through each facet joint were displayed. A sagittal cut through the middle of the facet joint was then referenced to analyze the 6 axial cuts and select the 3 axial cuts that best represented the cephalad, middle, and caudal aspects of the facet joint. After the 3 best axial cuts were chosen to grade, each was divided into thirds to represent the lateral 1/3, middle 1/3, and medial 1/3 of the facet joint at that level. Each area was then given a binary score of 0 or 1. A 0 was given if less than 50% of that area was bridged with bone. A 1 was given if bridging bone covered more than 50% of that area. The maximum score for any given axial image was 3 (>50% bridging bone across lateral 1/3, middle 1/3, and medial 1/3 of joint). The scores from the 3 axial images were added to get the patients’ TFFS. A TFFS of 9 would imply all three axial images were scored a 3. We considered a TFFS of > 4 was definitely fused, 3 was probably fused, and those with score <3 were considered not fused. The CT scans at 1-year and 2-year follow up were then compared to examine the rate and geographic progression of fusion over time.
Statistical Analysis
Wilcoxon-Sign-Rank test was used to test the differences in total scores between years. Mc- Nemar’s test was used to test if the distribution of fused versus nonfused/partially fused patients was different at the first year versus the second year. To explore the association between clinical outcomes and fusion scores, Spearman correlation was used. Software used for the analysis was SAS 9.2 (SAS Institute Inc.; Cary, NC, USA). Graphs were created using R 2.3.10 (The R Foundation; Vienna, Austria).
RESULTS
Of the 39 original subjects, sufficient vertebral imaging for scoring was available for 22 patients at 1 year and 37 patients at 2 years. Two subjects were excluded from scoring and analysis because of poor image quality and inadequate visualization of the facet joint. A single facet joint was evaluated in each patient, giving a total of 22 facet fusions at 1-year follow-up and 37 facet fusions at 2-year follow-up. First-year follow- up fusion scoring occurred at multiple anatomic levels including L3-L4 (1), L4-L5 (16), and L5-S1 (5). Second-year follow-up fusion scoring also occurred at L3-L4 (2), L4-L5 (27), and L5-S1 (8).
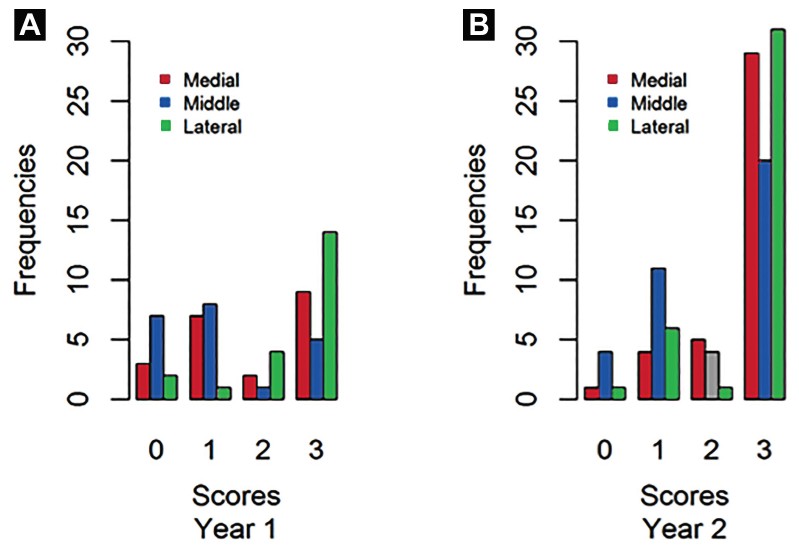
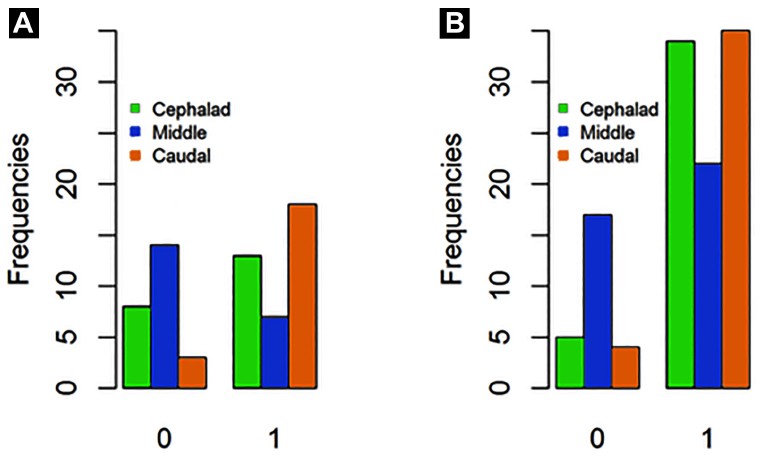
At 2 years, 89.74% of facet joints were considered definitely fused TFFS>4), compared with 71.43% at 1 year (p=0.04991). On axial CT views, the lateral aspect of the facet was seen to bridge most consistently by 1-year follow-up (90.91%) when compared with the middle (68.18%) and medial (86.36%) aspects. No significant progression of healing (p=0.06) was seen in the lateral region at the 2-year follow-up. The medial and middle aspects did show significant progression of healing by the 2-year follow- up (p=0.02 and p=0.004, respectively). On sagittal CT reconstructions, the caudal aspect of the facet was seen to bridge most consistently at 1-year follow-up (85.71%) compared with the middle (33.33%) and cephalad (61.90%) aspects. No significant progression of healing (p=0.2199) was seen in the caudal area of the joint between 1-year and 2-year follow-up. In comparison, the cephalad aspect of the facet joint showed significant (p=0.03103) progression of healing between 1-year and 2-year follow-up. The middle aspect of the facet showed the least amount of healing at 1 year, and there was no significant (p=0.1017) progression of healing at 2 year follow up. Clinical outcomes (VAS for back, leg, and ODI) were not associated with higher TFFS. However, only 19 patients had information on clinical outcomes and second-year scores; thus, this result may be biased.
Of the 39 original subjects, sufficient vertebral imaging for scoring was available for 22 patients at 1 year and 37 patients at 2 years. Two subjects were excluded from scoring and analysis because of poor image quality and inadequate visualization of the facet joint. A single facet joint was evaluated in each patient, giving a total of 22 facet fusions at 1-year follow-up and 37 facet fusions at 2-year follow-up. First-year follow- up fusion scoring occurred at multiple anatomic levels including L3-L4 (1), L4-L5 (16), and L5-S1 (5). Second-year follow-up fusion scoring also occurred at L3-L4 (2), L4-L5 (27), and L5-S1 (8).
At 2 years, 89.74% of facet joints were considered definitely fused TFFS>4), compared with 71.43% at 1 year (p=0.04991). On axial CT views, the lateral aspect of the facet was seen to bridge most consistently by 1-year follow-up (90.91%) when compared with the middle (68.18%) and medial (86.36%) aspects. No significant progression of healing (p=0.06) was seen in the lateral region at the 2-year follow-up. The medial and middle aspects did show significant progression of healing by the 2-year follow- up (p=0.02 and p=0.004, respectively). On sagittal CT reconstructions, the caudal aspect of the facet was seen to bridge most consistently at 1-year follow-up (85.71%) compared with the middle (33.33%) and cephalad (61.90%) aspects. No significant progression of healing (p=0.2199) was seen in the caudal area of the joint between 1-year and 2-year follow-up. In comparison, the cephalad aspect of the facet joint showed significant (p=0.03103) progression of healing between 1-year and 2-year follow-up. The middle aspect of the facet showed the least amount of healing at 1 year, and there was no significant (p=0.1017) progression of healing at 2 year follow up. Clinical outcomes (VAS for back, leg, and ODI) were not associated with higher TFFS. However, only 19 patients had information on clinical outcomes and second-year scores; thus, this result may be biased.
DISCUSSION
Traditional posterolateral fusion relies on an extensive bilateral dissection from midline to expose the intertransverse area in order to place graft and attempt to achieve a stable fusion. Often there is no specific preparation of the facet joint itself [8,9]. With the increased understanding of the negative consequences of a large posterolateral dissection, there has been a change in how some surgeons are attempting to achieve fusion, with less bone preparation and more use of expensive and powerful biologics such as BMP-2 [10]. This desire to improve or exceed open fusion rates with the use of biologicals is understandable, as there is substantial evidence that demonstrates the importance of obtaining a stable arthrodesis in order to maintain good long-term clinical outcomes [8,11-13]. If predictions regarding the increased use of minimally or less invasive surgeries (MIS, LIS) are correct, more information is needed to determine whether reliable facet fusion can be obtained with LIS techniques in the absence of extensive decortication. Since the patients in our TLIF studies had very little preparation of the facet joints, they represent an interesting cohort to assess whether decortication and grafting is required to obtain fusion through the facet joint.
In the late 1960s, orthopedic surgeons began studying why synovial joints would sometimes spontaneously fuse in the setting of external immobilization. These early investigations showed there are 2 separate histologic pathways that follow synovial joint immobilization, depending on whether the articular cartilage of the joints is in direct contact [2,14-16]. In absence of contact, an immobilized joint will first undergo capsular contraction and contraction of all soft tissue supporting structures. The joint cavity will then fill up with fibro-fatty tissue that slowly interfaces with the adjacent cartilaginous surfaces. Over time, the fibrofatty tissue will cause erosion through the cartilage surface and will eventually connect subchondral plate to subchondral plate in a fibrous type of union. A separate histologic process occurs in the presence of direct contact across the synovial joint. Compression leads to loss of nutrition to the areas under contact and rapid pressure necrosis of the articular cartilage. Microcystic changes occur throughout the articular cartilage and in the subchrondral plate. These microcysts eventually fill with mesenchymal tissue and vascular channels from the bone marrow. Enchondral ossification begins in these areas, eventually leading to bridging bone across the areas of compression [2,14-16]. Enneking & Horowitz confirmed this process in humans with a study of histologic changes seen in immobilized human knees in 1972 [14]. Baker et al. specifically studied the histologic changes seen in spinal facet joints after anterior arthrodesis and determined that the histology seen was similar to the changes seen in the above studies, but further noted that the changes seemed to start at the periphery of the facet joint where the articular surfaces are tightly opposed [2]. The results of this study support the above animal and clinical data suggesting facet joints reliably fuse in the absence of significant decortication when subject to immobilization and compression, as utilized in an open TLIF technique.
Our study also indicates that fusion starts at the periphery of the joint where the articular surfaces are more tightly opposed. Geographic grading revealed the most evidence of bridging bone at 1-year follow-up at the lateral and caudal areas: 90.91% and 85.71%, respectively. Statistically significant differences between 1-year and 2-year follow-up scores at the medial, middle, and cephalad aspects confirm the continuing progression of healing in these areas over time. This study supports previous studies demonstrating fusion beginning at the peripheral aspect of the joint, most commonly at the caudal aspect. Arthrodesis then proceeds in a cephalad direction along the sagittal plane. In this model, where no formal decortication of the articular surface was performed, the central portion of the joint showed less bridging bone at 1 year and the rate of complete fusion in the area did not increase at the 2-year follow-up.
Multiple methods of achieving facet joint fusion have been described in the literature, with fusion rates varying from 68%-97%, and at anywhere from 6 months to 2 years postoperatively [1,3,17-20]. These studies are very diverse in their techniques, with varying amounts of facet joint preparation, numerous types of bone grafting, and differing amounts of instrumentation and postoperative protocols. In addition, each study utilized different methods to determine presence of fusion and had different definitions for what they considered facet joint fusion. One of those authors, Kim et al., reported on the observed facet fusion rate seen after a standard lumbar intertransverse process fusion and noticed 68% of the facet joints spontaneously fused by CT at an average of 35 months postoperation [3]. Although their reported rate of fusion at greater than 2 years was slightly lower than the current study’s, their criteria used for confirming arthrodesis by CT was complete obliteration of joint space or trabecular bone bridging the entire facet joint space. Use of such strict criteria most likely accounts for their lower fusion rates. Had we used Kim’s criteria for fusion, our rate of fusion would have dropped to near 50% at the second year postoperative CT scan. Another study by Park et al. reported a 96% fusion rate at the 2-year follow-up confirmed with CT scan [1]. That study was in contrast to the current study in that it extensively debrided the cartilaginous endplates of the facet joints and packed the prepared joints with iliac crest autograft. Park et el. also used a less stringent definition for fusion. They considered fusion to be any bridging cancellous bone across the facet joint on either side of the body (right or left) [1]. By these criteria, we would have reported facet fusion in 100% of our patients in the current study, despite far less preparation of the facets. This study shows that in the setting of open TLIF surgery with compression across the facet joints, no formal preparation of the cartilaginous endplates of the facet is necessary to achieve facet fusion. When this is taken in the context of the previous literature, it is apparent that the bulk of basic science and clinical data suggest that rigid immobilization and compression at the facet joint can induce fusion in the majority of cases.
There are limitations to the current study worth discussing. While our results may be of interest to those using less invasive techniques to achieve facet joint fusion, our study was done with open technique, and the results may not be transferable to all MIS surgery. Another limitation of the study was the confounding effect from 3 possible fusion sites (interbody, intertransverse space, and facet) that would make it impossible to tell if the clinical results obtained were from the facet joint fusion or one of the other fusion sites. This study was not designed or powered to compare the clinical results amongst the 3 different sites. In addition, several previous studies have found no clinical advantage to fusion over pseudarthrosis in short-term studies. Therefore, the fact that there was no correlation between facet joint fusion and clinical results was not surprising. Finally, this study had a small sample size, and there is potential for selection bias. Even though the study was performed on prospectively collected data, the well-known limitations common to all retrospective studies apply.
Facet fusion reliably occurs after open TLIF and does not require decortication of the articular surface or powerful biologics when facet joints are stabilized with bilateral pedicle instrumentation. Spot welds at the caudal and lateral aspect of the facet joint are the most reliable CT-based indicator for facet fusions at 1-year follow-up. Bone bridging continues to progress in the cephalad direction, medially and centrally across the facet joints, between 1 and 2 years after the procedure. No correlation was seen between TFFS and clinical outcome. REFERENCES
[1]. Park Y-K, Kim J-H, Oh JI, Kwon T-H, Chung H-S, Lee K-C. Facet fusion in the lumbosacral spine: A 2-year follow-up study. Neurosurg. 2002;51:88-96.
[2] Baker WC, Thomas TG, Kirkaldy-Willis W. Changes in the cartilage of the posterior intervertebral joints after anterior fusion. J Bone Joint Surg Br. 1969;51:736-46.
[3] Kim NH, Lee JW. Anterior interbody fusion versus posterolateral fusion with transpedicular fixation for isthmic spondylolisthesis in adults. Spine. 1999;24:812-7.
[4] Kim C. Scientific Basis of Minimally Invasive Spine Surgery. Spine (Phila Pa 1976). 2010;35:S281-S286.
[5] Sihvonen T, Herno A, Paljärvi L, Airaksinen O, Partanen J, Tapaninaho A. Local denervation atrophy of paraspinal muscles in postoperative failed back syndrome. Spine (Phila Pa 1976). 1993;18:575-81.
[6] Oppenheimer J, DeCastro I, McDonnell D. Minimally invasive spine technology and minimally invasive spine surgery: a historical review. Neurosurg Focus. 2009;27:E9.
[7] Carter J, Swearingen A, Chaput C, Rahm M. Clinical and radiographic assessment of transforaminal lumbar interbody fusion using HEALOS collagen-hydroxyapatite sponge with autologous bone marrow aspirate. Spine J. 2009;9:434-8.
[8] Fischgrund J, Mackay M, Herkowitz H, Brower R, Montgomery D, Kurz L. Degenerative lumbar spondylolisthesis with spinal stenosis: a prospective, randomized study comparing decompressive laminectomy and arthrodesis with and without spinal instrumentation. Spine (Phila Pa 1976). 1997;22:2807-12.
[9] France J, Yaszemski M, Lauerman W, Cain J, Glover J, Lawson Kevin CJ, Topper S. A randomized prospective study of posterolateral lumbar fusion. Spine (Phil Pa 1976). 1999;24:553-60.
[10] Fineberg S, Ahmadinia K, Oglesby M, Patel A, Singh K. Hospital outcomes and complications of anterior and posterior cervical fusion with bone morphogenetic protein. Spine (Phila Pa 1976). 2013;38:1304-9.
[11] Deguchi M, Rapoff A, Zdeblick T. Posterolateral fusion for isthmic spondylolisthesis in adults. J Spinal Disord. 1998;11:459-64.
[12] Lenke L, Bridwell K, Bullis D, Betz R, Baldus C, Schoenecker P. Results of in situ fusion for isthmic spondylolisthesis. J Spinal Disord. 1992;5:433-42.
[13] Fischgrund J. The argument for instrumented decompressive posterolateral fusion for patients with degenerative spondylolisthesis and spinal stenosis. Spine (Phila Pa 1976). 2004;29:173-4.
[14] Enneking W, Morris JL. Human autologous cortical bone transplants. Clin Orthop Relat Res. 1972;87:28-35.
[15] Akeson W, Woo SL, Amiel D, Coutts R, Daniel D. The connective tissue response to immobility: biochemical changes in periarticular connective tissue of the immobilized rabbit knee. Clin Orthop Relat Res. 1973;93:356-62.
[16] Salter R, Field P. The effects of continuous compression on living articular cartilage: an experimental investigation. J Bone Joint Surg Am. 1960;42:31-90.
[17] Callahan R, Johnson R, Burke MR, Keggi K, Albright J, Southwick W. Cervical facet fusion for control of instability following laminectomy. J Bone Joint Surg Am. 1977;59:991-1002.
[18] Dai L-Y, Jiang L-S, Jiang S-D. Posterior short-segment fixation with or without fusion for thoracolumbar burst fractures. a five to seven-year prospective randomized study. J Bone Joint Surg Am. 2009;91:1033- 41.
[19] Jacobs RR, Montesano P, Jackson RP. Enhancement of lumbar spine fusion by use of translaminar facet joint screws. Spine (Phila Pa 1976). 1989;14:12-15.
[20] Stonecipher T, Wright S. Posterior lumbar interbody fusion with facet-screw fixation. Spine (Phila Pa 1976). 1989;14:468-71.
Traditional posterolateral fusion relies on an extensive bilateral dissection from midline to expose the intertransverse area in order to place graft and attempt to achieve a stable fusion. Often there is no specific preparation of the facet joint itself [8,9]. With the increased understanding of the negative consequences of a large posterolateral dissection, there has been a change in how some surgeons are attempting to achieve fusion, with less bone preparation and more use of expensive and powerful biologics such as BMP-2 [10]. This desire to improve or exceed open fusion rates with the use of biologicals is understandable, as there is substantial evidence that demonstrates the importance of obtaining a stable arthrodesis in order to maintain good long-term clinical outcomes [8,11-13]. If predictions regarding the increased use of minimally or less invasive surgeries (MIS, LIS) are correct, more information is needed to determine whether reliable facet fusion can be obtained with LIS techniques in the absence of extensive decortication. Since the patients in our TLIF studies had very little preparation of the facet joints, they represent an interesting cohort to assess whether decortication and grafting is required to obtain fusion through the facet joint.
In the late 1960s, orthopedic surgeons began studying why synovial joints would sometimes spontaneously fuse in the setting of external immobilization. These early investigations showed there are 2 separate histologic pathways that follow synovial joint immobilization, depending on whether the articular cartilage of the joints is in direct contact [2,14-16]. In absence of contact, an immobilized joint will first undergo capsular contraction and contraction of all soft tissue supporting structures. The joint cavity will then fill up with fibro-fatty tissue that slowly interfaces with the adjacent cartilaginous surfaces. Over time, the fibrofatty tissue will cause erosion through the cartilage surface and will eventually connect subchondral plate to subchondral plate in a fibrous type of union. A separate histologic process occurs in the presence of direct contact across the synovial joint. Compression leads to loss of nutrition to the areas under contact and rapid pressure necrosis of the articular cartilage. Microcystic changes occur throughout the articular cartilage and in the subchrondral plate. These microcysts eventually fill with mesenchymal tissue and vascular channels from the bone marrow. Enchondral ossification begins in these areas, eventually leading to bridging bone across the areas of compression [2,14-16]. Enneking & Horowitz confirmed this process in humans with a study of histologic changes seen in immobilized human knees in 1972 [14]. Baker et al. specifically studied the histologic changes seen in spinal facet joints after anterior arthrodesis and determined that the histology seen was similar to the changes seen in the above studies, but further noted that the changes seemed to start at the periphery of the facet joint where the articular surfaces are tightly opposed [2]. The results of this study support the above animal and clinical data suggesting facet joints reliably fuse in the absence of significant decortication when subject to immobilization and compression, as utilized in an open TLIF technique.
Our study also indicates that fusion starts at the periphery of the joint where the articular surfaces are more tightly opposed. Geographic grading revealed the most evidence of bridging bone at 1-year follow-up at the lateral and caudal areas: 90.91% and 85.71%, respectively. Statistically significant differences between 1-year and 2-year follow-up scores at the medial, middle, and cephalad aspects confirm the continuing progression of healing in these areas over time. This study supports previous studies demonstrating fusion beginning at the peripheral aspect of the joint, most commonly at the caudal aspect. Arthrodesis then proceeds in a cephalad direction along the sagittal plane. In this model, where no formal decortication of the articular surface was performed, the central portion of the joint showed less bridging bone at 1 year and the rate of complete fusion in the area did not increase at the 2-year follow-up.
Multiple methods of achieving facet joint fusion have been described in the literature, with fusion rates varying from 68%-97%, and at anywhere from 6 months to 2 years postoperatively [1,3,17-20]. These studies are very diverse in their techniques, with varying amounts of facet joint preparation, numerous types of bone grafting, and differing amounts of instrumentation and postoperative protocols. In addition, each study utilized different methods to determine presence of fusion and had different definitions for what they considered facet joint fusion. One of those authors, Kim et al., reported on the observed facet fusion rate seen after a standard lumbar intertransverse process fusion and noticed 68% of the facet joints spontaneously fused by CT at an average of 35 months postoperation [3]. Although their reported rate of fusion at greater than 2 years was slightly lower than the current study’s, their criteria used for confirming arthrodesis by CT was complete obliteration of joint space or trabecular bone bridging the entire facet joint space. Use of such strict criteria most likely accounts for their lower fusion rates. Had we used Kim’s criteria for fusion, our rate of fusion would have dropped to near 50% at the second year postoperative CT scan. Another study by Park et al. reported a 96% fusion rate at the 2-year follow-up confirmed with CT scan [1]. That study was in contrast to the current study in that it extensively debrided the cartilaginous endplates of the facet joints and packed the prepared joints with iliac crest autograft. Park et el. also used a less stringent definition for fusion. They considered fusion to be any bridging cancellous bone across the facet joint on either side of the body (right or left) [1]. By these criteria, we would have reported facet fusion in 100% of our patients in the current study, despite far less preparation of the facets. This study shows that in the setting of open TLIF surgery with compression across the facet joints, no formal preparation of the cartilaginous endplates of the facet is necessary to achieve facet fusion. When this is taken in the context of the previous literature, it is apparent that the bulk of basic science and clinical data suggest that rigid immobilization and compression at the facet joint can induce fusion in the majority of cases.
There are limitations to the current study worth discussing. While our results may be of interest to those using less invasive techniques to achieve facet joint fusion, our study was done with open technique, and the results may not be transferable to all MIS surgery. Another limitation of the study was the confounding effect from 3 possible fusion sites (interbody, intertransverse space, and facet) that would make it impossible to tell if the clinical results obtained were from the facet joint fusion or one of the other fusion sites. This study was not designed or powered to compare the clinical results amongst the 3 different sites. In addition, several previous studies have found no clinical advantage to fusion over pseudarthrosis in short-term studies. Therefore, the fact that there was no correlation between facet joint fusion and clinical results was not surprising. Finally, this study had a small sample size, and there is potential for selection bias. Even though the study was performed on prospectively collected data, the well-known limitations common to all retrospective studies apply.
Facet fusion reliably occurs after open TLIF and does not require decortication of the articular surface or powerful biologics when facet joints are stabilized with bilateral pedicle instrumentation. Spot welds at the caudal and lateral aspect of the facet joint are the most reliable CT-based indicator for facet fusions at 1-year follow-up. Bone bridging continues to progress in the cephalad direction, medially and centrally across the facet joints, between 1 and 2 years after the procedure. No correlation was seen between TFFS and clinical outcome. REFERENCES
[1]. Park Y-K, Kim J-H, Oh JI, Kwon T-H, Chung H-S, Lee K-C. Facet fusion in the lumbosacral spine: A 2-year follow-up study. Neurosurg. 2002;51:88-96.
[2] Baker WC, Thomas TG, Kirkaldy-Willis W. Changes in the cartilage of the posterior intervertebral joints after anterior fusion. J Bone Joint Surg Br. 1969;51:736-46.
[3] Kim NH, Lee JW. Anterior interbody fusion versus posterolateral fusion with transpedicular fixation for isthmic spondylolisthesis in adults. Spine. 1999;24:812-7.
[4] Kim C. Scientific Basis of Minimally Invasive Spine Surgery. Spine (Phila Pa 1976). 2010;35:S281-S286.
[5] Sihvonen T, Herno A, Paljärvi L, Airaksinen O, Partanen J, Tapaninaho A. Local denervation atrophy of paraspinal muscles in postoperative failed back syndrome. Spine (Phila Pa 1976). 1993;18:575-81.
[6] Oppenheimer J, DeCastro I, McDonnell D. Minimally invasive spine technology and minimally invasive spine surgery: a historical review. Neurosurg Focus. 2009;27:E9.
[7] Carter J, Swearingen A, Chaput C, Rahm M. Clinical and radiographic assessment of transforaminal lumbar interbody fusion using HEALOS collagen-hydroxyapatite sponge with autologous bone marrow aspirate. Spine J. 2009;9:434-8.
[8] Fischgrund J, Mackay M, Herkowitz H, Brower R, Montgomery D, Kurz L. Degenerative lumbar spondylolisthesis with spinal stenosis: a prospective, randomized study comparing decompressive laminectomy and arthrodesis with and without spinal instrumentation. Spine (Phila Pa 1976). 1997;22:2807-12.
[9] France J, Yaszemski M, Lauerman W, Cain J, Glover J, Lawson Kevin CJ, Topper S. A randomized prospective study of posterolateral lumbar fusion. Spine (Phil Pa 1976). 1999;24:553-60.
[10] Fineberg S, Ahmadinia K, Oglesby M, Patel A, Singh K. Hospital outcomes and complications of anterior and posterior cervical fusion with bone morphogenetic protein. Spine (Phila Pa 1976). 2013;38:1304-9.
[11] Deguchi M, Rapoff A, Zdeblick T. Posterolateral fusion for isthmic spondylolisthesis in adults. J Spinal Disord. 1998;11:459-64.
[12] Lenke L, Bridwell K, Bullis D, Betz R, Baldus C, Schoenecker P. Results of in situ fusion for isthmic spondylolisthesis. J Spinal Disord. 1992;5:433-42.
[13] Fischgrund J. The argument for instrumented decompressive posterolateral fusion for patients with degenerative spondylolisthesis and spinal stenosis. Spine (Phila Pa 1976). 2004;29:173-4.
[14] Enneking W, Morris JL. Human autologous cortical bone transplants. Clin Orthop Relat Res. 1972;87:28-35.
[15] Akeson W, Woo SL, Amiel D, Coutts R, Daniel D. The connective tissue response to immobility: biochemical changes in periarticular connective tissue of the immobilized rabbit knee. Clin Orthop Relat Res. 1973;93:356-62.
[16] Salter R, Field P. The effects of continuous compression on living articular cartilage: an experimental investigation. J Bone Joint Surg Am. 1960;42:31-90.
[17] Callahan R, Johnson R, Burke MR, Keggi K, Albright J, Southwick W. Cervical facet fusion for control of instability following laminectomy. J Bone Joint Surg Am. 1977;59:991-1002.
[18] Dai L-Y, Jiang L-S, Jiang S-D. Posterior short-segment fixation with or without fusion for thoracolumbar burst fractures. a five to seven-year prospective randomized study. J Bone Joint Surg Am. 2009;91:1033- 41.
[19] Jacobs RR, Montesano P, Jackson RP. Enhancement of lumbar spine fusion by use of translaminar facet joint screws. Spine (Phila Pa 1976). 1989;14:12-15.
[20] Stonecipher T, Wright S. Posterior lumbar interbody fusion with facet-screw fixation. Spine (Phila Pa 1976). 1989;14:468-71.