
The Relationship of Body Mass Index to Total Hip Arthroplasty Complications
Clayton Vaughan, MD¹; Matthew Jordan, MD¹; John Reilly, MPH¹; Daniel Jupiter, PhD²; Kindyle Brennan, PhD, PT¹; Kirby Hitt, MD¹; Christopher Chaput, MD¹
¹Department of Orthopaedic Surgery, Baylor Scott and White Health; Temple, TX, USA
²Office of Biostatistics, University of Texas Medical Branch; Galveston, TX, USA
Corresponding Author:Clayton Vaughan, MD, Department of Orthopaedic Surgery, Baylor Scott & White Health, 2401 S. 31st Street, MS-35-300, Temple, TX 76508; USA; Clayton.Vaughan@BSWHealth.org
DOI: 10.18600/toj.020107
INTRODUCTION
For the last 50 years, rates of obesity have been increasing and as such have received much attention in the literature. The Center for Disease Control reports that more than 1 out of 3 adults in the United States are obese, and this number is expected to continue to rise [1]. Obesity has been shown to be a mechanical factor influencing the initiation and progression of osteoarthritis of the hip and knee [2,3]. Consequently, according to Kurtz et al. [4], by 2030, in the United States, the number of annual primary total hip and total knee arthroplasty (THA, TKA) procedures is estimated to grow by 174% (to 572,000) and 673% (to 3.48 million), respectively. While THA represents the most common, successful, and predictable intervention for disabling hip arthritis, there remain a number of associated medical and surgical complications which lead to significant cost to the patient, hospital, and society as a whole. Thus, recent literature has sought to identify potential risk factors associated with complications following THA. Previous studies have provided evidence suggesting that high body mass index (BMI) is associated with increased operative time, venous thromboembolic events, superficial and deep wound infections, blood loss, and aseptic loosening [5]. Even so, a universal consensus does not exist regarding the relationship between BMI and complications following THA.
Furthermore, the majority of studies in this area focus on the obese, with little attention directed towards complications in the underweight (BMI<18.5). While the number of underweight patients is much smaller than the obese population, estimated to account for only 1.7%-2.3% of adults [5,6], it has been previously shown that these patients have an increased all-cause mortality compared to normal weight individuals, with more than 33,000 excess deaths per year [7,8]. It is our belief that both obese and underweight patients are at increased risk of postoperative complications following total hip replacement surgery, and that BMI represents a potentially modifiable risk factor in both of these patient populations prior to undergoing THA. Therefore, the present study sought to determine if a relationship exists between BMI and complication rates in patients undergoing total hip replacement surgery as well as to attempt to determine more definitive BMI levels at which the complication rates of THA significantly increase. MATERIALS & METHODS
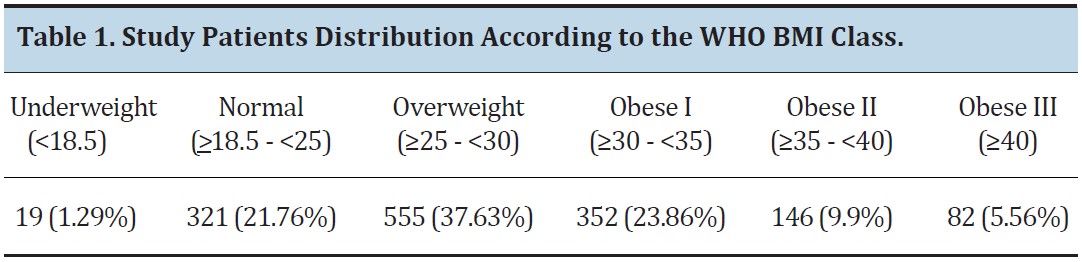
After approval was obtained from our institutional review board, a retrospective review was performed of 1,504 consecutive patients treated at a single institution from 2003 to 2011 by one of twelve board certified orthopedic surgeons. Data collected included patient’s age, gender, BMI, and types of complications. These complications were separated into surgical, medical, and any (surgical or medical) groups. Surgical complications were defined as wound complications, superficial wound infections, deep wound infections, DVT/PE, death, or other surgical complications (loose components, dislocation, or intraoperative fracture). For purposes of this study, a wound complication was defined as prolonged drainage, delayed healing, wound dehiscence, or formation of a seroma, hematoma, or stitch abscess; a superficial wound infection was defined as adjacent cellulitis or a deeper soft-tissue infection that did not communicate with the joint and was relieved with antibiotics +/- bedside/clinic debridement; and, finally, a deep-wound infection included any infection communicating with the joint confirmed by joint aspiration, positive intraoperative cultures, or frank purulence at the time of revision or antibiotic spacer placement. Medical complications were defined as pneumonia, cerebrovascular event, myocardial infarction, urinary tract infection, death or other medical complications (bladder infection, heel ulcer, fall causing injury, gastric ulcer, sepsis, gastrointestinal bleeding, renal failure, respiratory failure, or ileus). Surgical complications were limited to occurring within 3 months, postoperatively, while medical complications were noted up to 12 months, postoperatively. We used the World Health Organization (WHO) weight categorization for obesity: underweight (<18.5); normal (18.5 to <25); overweight (≥25 to <30); obese category I (≥30 to <35); obese Class II (≥35 to <40); and obese Class III (>40) [9]. The number of patients represented in each weight class is provided in Table 1.
For the last 50 years, rates of obesity have been increasing and as such have received much attention in the literature. The Center for Disease Control reports that more than 1 out of 3 adults in the United States are obese, and this number is expected to continue to rise [1]. Obesity has been shown to be a mechanical factor influencing the initiation and progression of osteoarthritis of the hip and knee [2,3]. Consequently, according to Kurtz et al. [4], by 2030, in the United States, the number of annual primary total hip and total knee arthroplasty (THA, TKA) procedures is estimated to grow by 174% (to 572,000) and 673% (to 3.48 million), respectively. While THA represents the most common, successful, and predictable intervention for disabling hip arthritis, there remain a number of associated medical and surgical complications which lead to significant cost to the patient, hospital, and society as a whole. Thus, recent literature has sought to identify potential risk factors associated with complications following THA. Previous studies have provided evidence suggesting that high body mass index (BMI) is associated with increased operative time, venous thromboembolic events, superficial and deep wound infections, blood loss, and aseptic loosening [5]. Even so, a universal consensus does not exist regarding the relationship between BMI and complications following THA.
Furthermore, the majority of studies in this area focus on the obese, with little attention directed towards complications in the underweight (BMI<18.5). While the number of underweight patients is much smaller than the obese population, estimated to account for only 1.7%-2.3% of adults [5,6], it has been previously shown that these patients have an increased all-cause mortality compared to normal weight individuals, with more than 33,000 excess deaths per year [7,8]. It is our belief that both obese and underweight patients are at increased risk of postoperative complications following total hip replacement surgery, and that BMI represents a potentially modifiable risk factor in both of these patient populations prior to undergoing THA. Therefore, the present study sought to determine if a relationship exists between BMI and complication rates in patients undergoing total hip replacement surgery as well as to attempt to determine more definitive BMI levels at which the complication rates of THA significantly increase. MATERIALS & METHODS
After approval was obtained from our institutional review board, a retrospective review was performed of 1,504 consecutive patients treated at a single institution from 2003 to 2011 by one of twelve board certified orthopedic surgeons. Data collected included patient’s age, gender, BMI, and types of complications. These complications were separated into surgical, medical, and any (surgical or medical) groups. Surgical complications were defined as wound complications, superficial wound infections, deep wound infections, DVT/PE, death, or other surgical complications (loose components, dislocation, or intraoperative fracture). For purposes of this study, a wound complication was defined as prolonged drainage, delayed healing, wound dehiscence, or formation of a seroma, hematoma, or stitch abscess; a superficial wound infection was defined as adjacent cellulitis or a deeper soft-tissue infection that did not communicate with the joint and was relieved with antibiotics +/- bedside/clinic debridement; and, finally, a deep-wound infection included any infection communicating with the joint confirmed by joint aspiration, positive intraoperative cultures, or frank purulence at the time of revision or antibiotic spacer placement. Medical complications were defined as pneumonia, cerebrovascular event, myocardial infarction, urinary tract infection, death or other medical complications (bladder infection, heel ulcer, fall causing injury, gastric ulcer, sepsis, gastrointestinal bleeding, renal failure, respiratory failure, or ileus). Surgical complications were limited to occurring within 3 months, postoperatively, while medical complications were noted up to 12 months, postoperatively. We used the World Health Organization (WHO) weight categorization for obesity: underweight (<18.5); normal (18.5 to <25); overweight (≥25 to <30); obese category I (≥30 to <35); obese Class II (≥35 to <40); and obese Class III (>40) [9]. The number of patients represented in each weight class is provided in Table 1.
Statistical Analysis
The relationships between age, gender, BMI and the occurrence of complications postoperatively were examined utilizing t-tests or χ-squared/Fisher’s exact tests, as appropriate. The data were analyzed for each type of complication individually and within the following groups: any complications (surgical or medical), surgical complications (as defined above), and medical complications (as defined above).
The relationships between age, gender, BMI and the occurrence of complications postoperatively were examined utilizing t-tests or χ-squared/Fisher’s exact tests, as appropriate. The data were analyzed for each type of complication individually and within the following groups: any complications (surgical or medical), surgical complications (as defined above), and medical complications (as defined above).
These relationships were assessed using BMI either as a raw number or by the WHO stratifications as described. Logistic regression for each group of complications was performed, including covariates age, gender, and either BMI or stratified BMI. In addition, cut-off points (break points) were sought in an attempt to determine at what BMI levels did the incidence of complications change dramatically.
This analysis was performed using segmented regression and multivariate adaptive regression splines (MARS®; Salfort System, San Diego, Ca), both of which required 'instantaneous' complication rates, as follows: for each patient, BMI levels were examined; we then found those patients whose BMI levels were within 10 larger or 10 smaller than that of the original patient; finally, the patient was assigned the rate of complication of all the patients thus discovered The goal was to determine if a linear relationship, either globally or locally, existed between BMI and the rate of complications, or whether there were points at which behavior changed drastically.
RESULTS
The study population consisted of 1,475 patients (29 excluded had either missing data or lost follow-up). The mean age was 66.1 years (19-95 years). The mean age (years) for each BMI class was as follows: underweight 63.9; normal 67.8; overweight 67.8; obesity class I 65.1, obesity class II 61.7; obesity class III 60.8. The average BMI was 29.2 (standard deviation 5.86). Men had an average BMI of 29.8 (standard deviation 5.29), while women had an average BMI of 28.7 (standard deviation 6.23), (p<0.001). There were 276 (18.69%) any complications, 161 (10.90%) surgical complications, and 137 (9.28%) medical complications. The incidences of all complications are shown in Table 2.
Any Complications (Surgical or Medical)
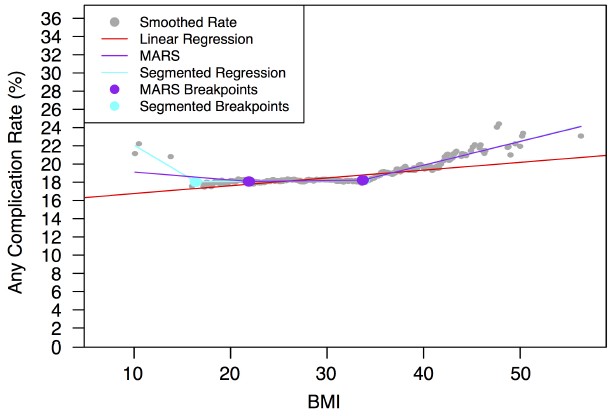
There were 276 (18.69%) patients with either a surgical or a medical complication. These patients with any complications had a mean age of 68.7, compared to those patients without a complication who had a mean age of 65.5 (p<0.001). There was no difference between genders in term of rates of complications (χ-squared; p=0.11). In addition, BMI did not significantly differ between those with or without a complication by either t-test (p=0.47) or Fisher’s exact test. Multivariate analysis revealed a relationship between age and the rate of any complications, with an odds ratio (OR) of 1.02 (95%CI: 1.01-1.03) for each additional year of age. Multivariate analyses also revealed a U-shaped trend, with more complications occurring at the extremes of BMI (both low and high), and with break points at BMI 21.9 and 33.7, respectively. A similar trend was also seen using segmented regression, with breakpoints at 16.4 and 33.81 (Figure 1).
The study population consisted of 1,475 patients (29 excluded had either missing data or lost follow-up). The mean age was 66.1 years (19-95 years). The mean age (years) for each BMI class was as follows: underweight 63.9; normal 67.8; overweight 67.8; obesity class I 65.1, obesity class II 61.7; obesity class III 60.8. The average BMI was 29.2 (standard deviation 5.86). Men had an average BMI of 29.8 (standard deviation 5.29), while women had an average BMI of 28.7 (standard deviation 6.23), (p<0.001). There were 276 (18.69%) any complications, 161 (10.90%) surgical complications, and 137 (9.28%) medical complications. The incidences of all complications are shown in Table 2.
Any Complications (Surgical or Medical)
There were 276 (18.69%) patients with either a surgical or a medical complication. These patients with any complications had a mean age of 68.7, compared to those patients without a complication who had a mean age of 65.5 (p<0.001). There was no difference between genders in term of rates of complications (χ-squared; p=0.11). In addition, BMI did not significantly differ between those with or without a complication by either t-test (p=0.47) or Fisher’s exact test. Multivariate analysis revealed a relationship between age and the rate of any complications, with an odds ratio (OR) of 1.02 (95%CI: 1.01-1.03) for each additional year of age. Multivariate analyses also revealed a U-shaped trend, with more complications occurring at the extremes of BMI (both low and high), and with break points at BMI 21.9 and 33.7, respectively. A similar trend was also seen using segmented regression, with breakpoints at 16.4 and 33.81 (Figure 1).
Surgical Complications
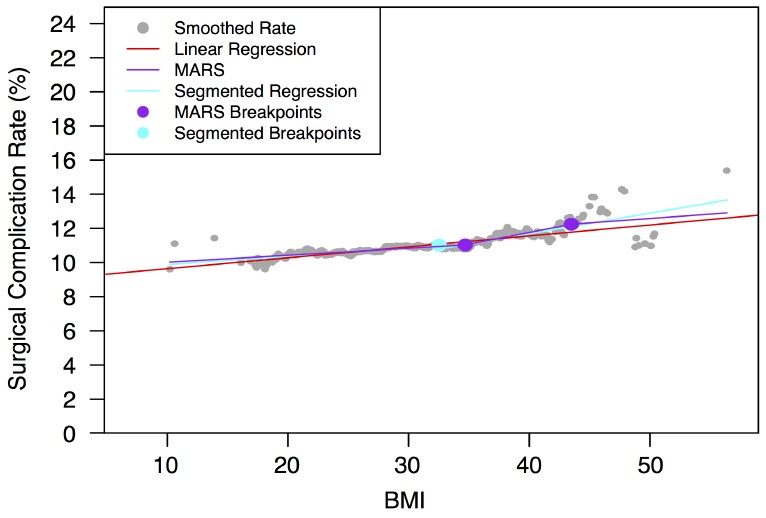
One hundred sixty-one (10.9%) patients experienced a surgical complication in our study population. Bivariate analysis did not reveal a relationship between age, gender, or BMI and the presence of surgical complications upon t-test (p=0.29), χ-squared test (p=0.94), or t-test (p=0.40), respectively. Likewise, there was no relationship between age, gender, or BMI and the presence of surgical complications upon multivariate analysis. However, while it did not reach the level of statistical significance, there was a trend demonstrating an increased rate of deep wound infections in both the underweight (5.26%) and the obesity Class II (6.85%) and III (4.88%) groups, which mirrored the previously seen U-shaped trend found in the any complications analysis (Figure 2).
Medical Complications
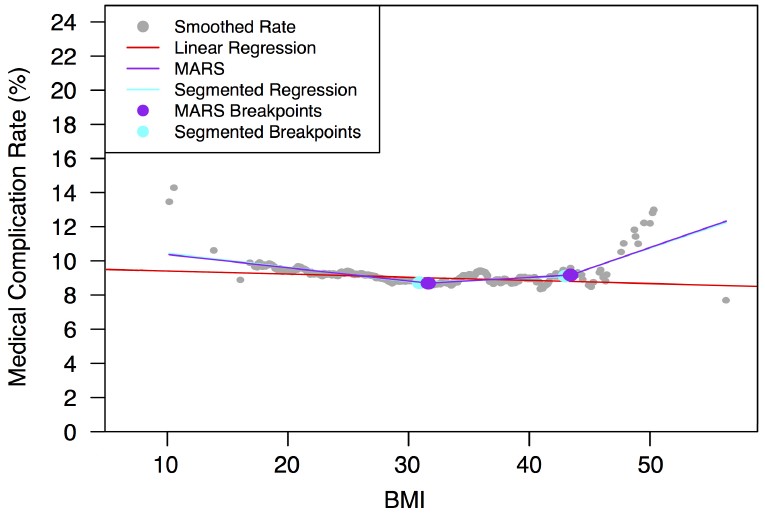
One hundred and thirty-seven (9.28%) patients experienced a medical complication. These patients had a mean age of 71.3, compared to those without a medical complication who had an average age of 65.6 (p<0.001). Of women, 10.84% experienced a medical complication versus 7.26% of men (p=0.019). While BMI did not significantly differ between those with or without a medical complication on bivariate analysis (p=0.64), multivariate analysis did reveal an association between increased medical complications in the underweight and obesity Class III groups, as well as with each year of increasing age. The underweight class showed the strongest association with medical complications (OR=4.29; 95%CI: 1.36-13.5), versus the obesity Class III (OR= 2.32; 95%CI: 1.05-5.17) versus each additional year of age (OR=1.04; 95%CI: 1.02-1.06) (Figure 3).
One hundred sixty-one (10.9%) patients experienced a surgical complication in our study population. Bivariate analysis did not reveal a relationship between age, gender, or BMI and the presence of surgical complications upon t-test (p=0.29), χ-squared test (p=0.94), or t-test (p=0.40), respectively. Likewise, there was no relationship between age, gender, or BMI and the presence of surgical complications upon multivariate analysis. However, while it did not reach the level of statistical significance, there was a trend demonstrating an increased rate of deep wound infections in both the underweight (5.26%) and the obesity Class II (6.85%) and III (4.88%) groups, which mirrored the previously seen U-shaped trend found in the any complications analysis (Figure 2).
Medical Complications
One hundred and thirty-seven (9.28%) patients experienced a medical complication. These patients had a mean age of 71.3, compared to those without a medical complication who had an average age of 65.6 (p<0.001). Of women, 10.84% experienced a medical complication versus 7.26% of men (p=0.019). While BMI did not significantly differ between those with or without a medical complication on bivariate analysis (p=0.64), multivariate analysis did reveal an association between increased medical complications in the underweight and obesity Class III groups, as well as with each year of increasing age. The underweight class showed the strongest association with medical complications (OR=4.29; 95%CI: 1.36-13.5), versus the obesity Class III (OR= 2.32; 95%CI: 1.05-5.17) versus each additional year of age (OR=1.04; 95%CI: 1.02-1.06) (Figure 3).
DISCUSSION
Despite recent interest and research in this area of orthopedics, there continues to be some controversy surrounding the precise relationship between BMI and the risk of complications following total hip replacement surgery. Some authors argue that there is not an increase in complications [10-13], while others suggest there is [14-20]. Given the epidemic of obesity in the United States, much of the existing literature has focused on evaluating perioperative complications in this growing population. Less is therefore known about the potential sequelae of being underweight in patients undergoing THA. Our belief is that both the underweight and obese patient populations are at increased risk for postoperative complications following total hip replacement surgery.
In this large series of patients, our data revealed increased rates of medical complications in both the “underweight” and “obese Class III” populations as compared to normal weight patients; the underweight population showed the strongest association with development of a medical complication. This finding regarding underweight patients is in agreement with those by Alfonso et al. [5] who first reported that these patients might be susceptible to increased complications following total hip replacement surgery. In their study, these complications included higher rates of blood transfusions and dislocations. Similar trends have also been reported in the general surgery literature—with increased rates of postoperative complications and even early mortality in underweight patients undergoing coronary artery bypass surgery [21,22].
Additionally, we observed a trend of an increased rate of any complications among patients at the extremes of BMI. Similar U-shaped trends have previously been reported following both THA [17-19] as well as coronary artery bypass surgery [21]. In 2009 Marks et al. [17] evaluated 1,040 patients undergoing either primary or revision THA and reported more dislocations in underweight patients (p<0.05) and higher rates of prosthetic loosening, periprosthetic fractures, and deep infections in the high BMI group (p=0.07). In 2012, Zhang et al. [18] found increased rates of both overall complications (18.4%) and dislocations (10.5%, p=0.041) in underweight patients, as well as a higher rate of DVTs (6.1%; p=0.053) in the obese group. Most recently, Murgatroyd et al. [19] evaluated 5,357 patients from the New Zealand Joint Registry who underwent primary THA, with 2% of these patients being underweight.
Although they defined underweight as having a BMI<20 versus the more widely accepted WHO classification of <18.5, their study also revealed a similar U-shaped trend, with higher revision rates along with lower Oxford Hip scores in both the underweight and obese groups. Although not statistically significant, our data also revealed a trend with higher rates of deep infections in both the underweight (5.26%) and obese Class I, II, III (3.13%, 6.85%, 4.88%) patient populations. These rates are much higher than previously reported in primary THA literature [23], as well as when compared to the deep infection rate in our normal BMI class (2.18%). Previous studies have reported similar trends [23-25]. Dowsey et al. [23] showed that BMI is a risk factor for deep infections following THA, independent of patient comorbidities, such as diabetes and cardiovascular disease: 2.6% of obese patients and 9.1% of morbidly obese patients developed an acute prosthetic infection, compared with 1.0% in the normal weight range. The most common medical complication in our study was urinary tract infections (UTIs), which also occurred more frequently in the underweight and morbidly obese populations. This particular catheter-related complication has recently drawn much attention [26], with many institutions now having implemented programs aimed at decreasing the incidence of catheter-related UTIs in hospitalized patients. At our institution, we initiated a new protocol limiting Foley catheter insertion on arthroplasty patients and requiring daily physician renewal orders for these catheters. Knoll et al. [27] showed a 15-fold decrease in the use of unnecessary Foley catheters using an institution-wide protocol, such as ours.
Our study highlights another important consideration when evaluating the association between BMI and complications after total hip replacement surgery. Many studies comparing obese and nonobese patients include the underweight (BMI <18.5) population as part of the nonobese cohort [28,29]. For instance, Leahy [29] reported similar functional outcomes and complication rates in obese patients undergoing total knee arthroplasty compared to non-obese patients. The patients were separated into 3 comparison groups: 1) BMI 15-24.9; 2) BMI 25-39.9; and 3) BMI 40-60. Group 1 includes both normal BMI as well as underweight patients. Our study has shown an increased risk of medical complications in the underweight—a finding that is in agreement with another previously published report [5]. Therefore, not separating these cohorts may potentially underestimate the difference in complication rates between obese and 'normal' BMI patient populations.
Finally, having a BMI of less than 18.5 may simply reflect a state of malnourishment or may be the manifestation of an underlying disease process, such as malignancy, infection, inflammatory disorders, psychiatric disorders, or other congenital conditions. The musculoskeletal sequelae of being underweight often include decreased muscle mass, decreased soft tissue mass, as well as a higher incidence of osteoporosis [5]. These factors are not inconsequential considerations for the orthopedic surgeon performing total hip replacement surgery, as previous studies have demonstrated higher rates of dislocations in underweight patients compared to normal weight individuals [5,17,18]. We believe this finding is likely due to these patients’ decreased muscle mass and soft tissue tension around the hip joint associated with their underweight status.
We recognize that the present study has certain limitations—most notably that it is a retrospective review, with all of the attendant limitations including reliance on the accuracy and completeness of hospital records within our electronic database. Another limitation is the relatively low number of underweight patients, representing 1.29% of our study population. While this incidence falls slightly below the most recent estimated national prevalence of 1.7% [6], it does represent a larger percentage of underweight patients than found within the first study reporting increased complications in this group where only 0.46% of their patients were underweight [5]. An additional limitation is that we did not specifically control for other comorbidities, such as diabetes, cardiovascular disease, or smoking. The present study does not claim that BMI is an independent risk factor for THA complications, and it is likely that patients with both high and low BMI have associated comorbidities that play a role in their complications. It is well understood that BMI has significant limitations as a predictor, and we simply wanted to see if there were increased complications in both high and low BMI patients that had not been previously reported. A larger dataset, preferably multicenter, would be required to appropriately control for comorbid conditions and assess the existence of an independent association.
As mentioned above, there are also certain limitations to BMI in and of itself. One of these limitations is that BMI may simply be a surrogate marker for nutritional status, as obese patients can often have paradoxical malnutrition. While BMI may represent an indirect measure of nutritional status, studies have shown that albumin may actually be a better predictor than BMI of outcomes after coronary artery bypass surgery [30]. Future studies are needed to examine a larger population of underweight and obese patients undergoing THA, specifically looking at nutritional status/indices and other metabolic factors that may also contribute to postoperative complications. Similarly, there is the inability of BMI to distinguish adiposity from lean mass [31]. BMI is a quick and easy indicator of excess adiposity; however, the accuracy varies according to the relative amounts of adiposity and lean mass [32,33]. Mehta et al. [34] recently showed how weight distribution is more strongly associated with infection risk than BMI in patients undergoing lumbar spinal fusion surgery. Future studies may use a more accurate assessment of true body mass and perhaps include screens for metabolic risk factors associated with obesity, such as metabolic syndrome. Indeed, metabolic syndrome and its relationship to total joint arthroplasty have started to gain attention [26,35]. Gonzales et al. [35] showed that metabolic syndrome was an independent risk factor for the development of major complications, nonroutine discharge, and increased hospital cost in patients undergoing total hip and knee arthroplasty. Likewise, Saucedo et al. [36] found a U-shaped trend relating underweight and obese patient populations to an increased cost associated with post-operative complications, reporting that low BMI was an independent risk factor for readmission within 90 days following THA, and that a high BMI was significant for readmission within 30 days following total knee arthroplasty surgery. These findings, along with those of the present study, provide further evidence that these 2 patient populations are at increased risk for postoperative complications; thus, representing a significant financial burden to the patient, hospital, and society as a whole. In today’s rapidly changing healthcare environment, hospitals and physicians face increasing pressure to decrease surgical and medical complications that lead to higher cost. By understanding how BMI may affect our outcomes, we can attempt to influence this potentially modifiable risk factor preoperatively to help reduce costs related to postoperative complications. CONCLUSIONS
This study further indicates the increased rate of medical complications for patients with both high and low BMI who undergo primary THA. Given the rising cost of healthcare, it is important to recognize the association between postoperative complications in both the obese and underweight patient populations. Future studies to better define the relationship between underweight patients and postoperative complications are needed, as this is a small, but not insignificant, subset of arthroplasty patients. REFERENCES
[1] Ogden C, Carroll M, Kit B, Flegal K (2012) Prevalence of Obesity in the United States 2009-2010. NCHS data brief, no 82. Hyattsville, MD: National Center for Health Statistics. 2012.
[2] Hohmander LS, Gerhardsson de Verdier M, Rollof J. Incidence of severe knee and hip osteoarthritis in relation to different measures of body mass: a population-based prospective cohort study. Ann Rheum Dis. 2009;68:490-6.
[3] Järvholm B, Lewold S, Malchau H, Vingård E. Age, bodyweight, smoking habits and the risk of severe osteoarthritis in the hip and knee in men. Eur J Epidemiol. 2005;20:537-42.
[4] Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89:780-5.
[5] Alfonso DT, Howell RD, Caceres G, Kozlowski P, DiCesare PE. Total hip arthroplasty in the underweight. J Arthroplasty. 2008;23:956-9.
[6] Fryar CD, Ogden CL. Prevalence of underweight among adults aged 20 years and over: United States, 1960-1962 through 2007-2010. Available at: http://www.cdc.gov/nchs/data/hestat/underweight_adult_07_10/underweight_adult_07_10.pdf
[7] Flegal KM, Graubard BI, Williamson DF, Gail MH. Excess deaths associated with underweight, overweight, and obesity. JAMA. 2005;293:1861-7.
[8] Ringback WG, Eliasson M, Rosen M. Underweight, overweight and obesity as risk factors for mortality and hospitalization. Scand J Public Health. 2008;36:169-76.
[9] World Health Organization. BMI Classification. http://apps.who.int/bmi/index.jsp?introPage=intro_3.html
[10] Luleiman LI, Orgeta G, Onguti S, Gonzalez DO, Tran DD, Onyike A, Turner PL, Fullum TM. Does BMI affect perioperative complications following total knee and hip arthroplasty? J Surg Res. 2012;174:7-11.
[11] Moran M, Walmsley P, Gray A, Brenkel IJ. Does body mass index affect the early outcome of primary total hip arthroplasty? J Arthroplasty. 2005;20:866-9.
[12] Jiganti JJ, Goldstein WM, Williams CS. A comparison of the perioperative morbidity in total joint arthroplasty in the obese and non-obese patient. Clin Orthop Relat Res. 1993;289: 175-9.
[13] Suleiman LI, Ortega G, Ong'uti SK, Gonzalez DO, Tran DD, Onyike A, Turner PL, Fullum TM. Does BMI affect perioperative complications following total knee and hip arthroplasty? J Surg Res. 2012;174:7-11.
[14] Namba RS, Paxton L, Fithian DC, Stone ML. Obesity and perioperative morbidity in total hip and total knee arthroplasty patients. J Arthroplasty. 2005;20:46-50.
[15] Jain NB, Guller U, Pietrobon R, Bond TK, Higgins LD. Comorbidities increase complication rates in patients having arthroplasty. Clin Orthop Relat Res. 2005;435:232-8.
[16] Chee JH, Teoh KH, Sabnis BM, Ballantyne JA, Brenkel IJ. Total hip replacement in morbidly obese patients with osteoarthritis. J Bone Joint Surg Br. 2010;92B:1066-71.
[17] Marks R. Body mass characteristics of hip osteoarthritis patients experiencing aseptic loosening, periprosthetic fractures, dislocation, and infections after total hip replacement. Clinicoecon Outcomes Res. 2009;1:7-16
[18] Zhang ZJ, Zhao XY, Kang Y, Zhang ZQ, Yang ZB, He AS, Fu M, Sheng PY, Liao WM. The influence of body mass index on life quality and clinical improvement after total hip arthroplasty. J Orthop Sci. 2012;17:219-25.
[19] Murgatroyd SE, Frampton CM, Wright MS. The effect of body mass index on outcome in total hip arthroplasty: early analysis from the New Zealand joint registry. J Arthroplasty. 2014;29:1884-8.
[20] Sabharwal S, Root MZ. Impact of obesity on orthopaedics. J Bone joint Surg Am. 2012;94:1045-52.
[21] Wagner BD, Grunwald GK, Rumsfeld JS, Hill JO, Ho PM, Wyatt HR, Shroyer AL. Relationship of body mass index with outcomes after coronary artery bypass graft surgery. Ann Thorac Surg. 2007;84:10-6.
[22] Atalan N, Fazlioqullan O, Kunt AT, Basaran C, Gurer O, Sitilci T, Akqun S, Arsan S. Effect of body mass index on early morbidity and mortality after isolated coronary artery bypass graft surgery. J Cardiothorac Vasc Anesth. 2012;26:813-7.
[23] Dowsey MM, Choong FM. Obesity is a major risk factor for prosthetic infection after primary hip arthroplasty. Clin Orthop Relat Res. 2008;466:153-8.
[24] Malinzak RA, Ritter MA, Berend ME, Meding JB, Olberding EM, Davis KE. Morbidly obese, diabetic, younger, and unilateral joint arthroplasty patients have elevated total joint arthroplasty infection rates. J Arthroplasty. 2009;24:84-8.
[25] Jamsen E, Nevalainen P, Eskelinen A, Huotari K, Kalliovalkama J, Moilanen T. Obesity, diabetes, and preoperative hyperglycemia as predictors of periprosthetic joint infection. J Bone Joint Surg Am. 2012;94:e101.
[26] Miller RS, Norris PR, Jenkins JM, Talbot TR, Starmer JM, Hutchison SA, Carr DS, Kleymeer CJ, Morris JA. Systems initiatives reduce healthcare-associated infections; a study of 22,928 device days in a single trauma unit. J Trauma. 2010;68:23-31.
[27] Knoll BM, Wright D, Ellingson L, Kraemer L, Patire R, Kuskowski MA, Johnson JR. Reduction of inappropriate urinary catheter use at a veterans affairs hospital through a multifaceted quality improvement project. Clin Infect Dis. 2011;52:1283-90.
[28] Patel AD, Albrizio M. Relationship of body mass index to early complications in knee replacement surgery. Arch Orthop Trauma Surg. 2008;128:5-9.
[29] Leahy, M. TKA improves function regardless of patient’s BMI. AAOS Now. October 2012.
[30] Bhamidipati CM, LaPar DJ, Mehta GS, Kern JA, Upchurch GR Jr, Kron IL, Ailawadi G. Albumin is a better predictor of outcomes than body mass index following coronary artery bypass grafting. Surgery. 2011;150:626-34.
[31] Ferguson DF, Busenlehner BJ, Rahm MD, Mehta SM, Song J, Davis ML, Sampson W, Chaput CD. The use of routine thoracoabdominal CT scans in the polytrauma patient to estimate obesity. Obesity. 2012;21:997-1003.
[32] Okorodudu DO, Jumean MF, Montori VM, Romero-Corral A, Somers VK, Erwin PJ, Lopez-Jimenez F. Diagnostic performance of body mass index to identify obesity as defined by body adiposity: a systematic review and meta-analysis. Int J Obes. 2010;34:791-9.
[33] Romero-Corral A, Somers VK, Sierra-Johnson J, Thomas RJ, Collazo-Clavell ML, Korinek J, Allison TG, Batsis JA, Sert-Kuniyoshi FH, Lopez-Jimenez F. Accuracy of body mass index in diagnosing obesity in the adult general population. Int J Obes (Lond) 2008;32:959-6.
[34] Mehta AI, Babu R, Karikari IO, Grunch B, Agarwal VJ, Owens TR, Friedman AH, Bagley CA, Gottfried ON. The distribution of body mass as a significant risk factor for lumbar spinal fusion postoperative infections. Spine. 2012;37: 1652-6.
[35] Gonzalez Della Valle AG, Chiu YL, Ma Y, Mazumdar M, Memtsoudis SG. The metabolic syndrome in patients undergoing knee and hip arthroplasty: trends and in-hospital outcomes in the United States. J Arthroplasty. 2012;27:1743-9.
[36] Saucedo JM, Marecek GS, Wanke TR, Lee J, Stulberg SD, Puri L. Understanding readmission after primary total hip and knee arthroplasty: who’s at risk? J Arthroplasty. 2014;29:256-60.
Despite recent interest and research in this area of orthopedics, there continues to be some controversy surrounding the precise relationship between BMI and the risk of complications following total hip replacement surgery. Some authors argue that there is not an increase in complications [10-13], while others suggest there is [14-20]. Given the epidemic of obesity in the United States, much of the existing literature has focused on evaluating perioperative complications in this growing population. Less is therefore known about the potential sequelae of being underweight in patients undergoing THA. Our belief is that both the underweight and obese patient populations are at increased risk for postoperative complications following total hip replacement surgery.
In this large series of patients, our data revealed increased rates of medical complications in both the “underweight” and “obese Class III” populations as compared to normal weight patients; the underweight population showed the strongest association with development of a medical complication. This finding regarding underweight patients is in agreement with those by Alfonso et al. [5] who first reported that these patients might be susceptible to increased complications following total hip replacement surgery. In their study, these complications included higher rates of blood transfusions and dislocations. Similar trends have also been reported in the general surgery literature—with increased rates of postoperative complications and even early mortality in underweight patients undergoing coronary artery bypass surgery [21,22].
Additionally, we observed a trend of an increased rate of any complications among patients at the extremes of BMI. Similar U-shaped trends have previously been reported following both THA [17-19] as well as coronary artery bypass surgery [21]. In 2009 Marks et al. [17] evaluated 1,040 patients undergoing either primary or revision THA and reported more dislocations in underweight patients (p<0.05) and higher rates of prosthetic loosening, periprosthetic fractures, and deep infections in the high BMI group (p=0.07). In 2012, Zhang et al. [18] found increased rates of both overall complications (18.4%) and dislocations (10.5%, p=0.041) in underweight patients, as well as a higher rate of DVTs (6.1%; p=0.053) in the obese group. Most recently, Murgatroyd et al. [19] evaluated 5,357 patients from the New Zealand Joint Registry who underwent primary THA, with 2% of these patients being underweight.
Although they defined underweight as having a BMI<20 versus the more widely accepted WHO classification of <18.5, their study also revealed a similar U-shaped trend, with higher revision rates along with lower Oxford Hip scores in both the underweight and obese groups. Although not statistically significant, our data also revealed a trend with higher rates of deep infections in both the underweight (5.26%) and obese Class I, II, III (3.13%, 6.85%, 4.88%) patient populations. These rates are much higher than previously reported in primary THA literature [23], as well as when compared to the deep infection rate in our normal BMI class (2.18%). Previous studies have reported similar trends [23-25]. Dowsey et al. [23] showed that BMI is a risk factor for deep infections following THA, independent of patient comorbidities, such as diabetes and cardiovascular disease: 2.6% of obese patients and 9.1% of morbidly obese patients developed an acute prosthetic infection, compared with 1.0% in the normal weight range. The most common medical complication in our study was urinary tract infections (UTIs), which also occurred more frequently in the underweight and morbidly obese populations. This particular catheter-related complication has recently drawn much attention [26], with many institutions now having implemented programs aimed at decreasing the incidence of catheter-related UTIs in hospitalized patients. At our institution, we initiated a new protocol limiting Foley catheter insertion on arthroplasty patients and requiring daily physician renewal orders for these catheters. Knoll et al. [27] showed a 15-fold decrease in the use of unnecessary Foley catheters using an institution-wide protocol, such as ours.
Our study highlights another important consideration when evaluating the association between BMI and complications after total hip replacement surgery. Many studies comparing obese and nonobese patients include the underweight (BMI <18.5) population as part of the nonobese cohort [28,29]. For instance, Leahy [29] reported similar functional outcomes and complication rates in obese patients undergoing total knee arthroplasty compared to non-obese patients. The patients were separated into 3 comparison groups: 1) BMI 15-24.9; 2) BMI 25-39.9; and 3) BMI 40-60. Group 1 includes both normal BMI as well as underweight patients. Our study has shown an increased risk of medical complications in the underweight—a finding that is in agreement with another previously published report [5]. Therefore, not separating these cohorts may potentially underestimate the difference in complication rates between obese and 'normal' BMI patient populations.
Finally, having a BMI of less than 18.5 may simply reflect a state of malnourishment or may be the manifestation of an underlying disease process, such as malignancy, infection, inflammatory disorders, psychiatric disorders, or other congenital conditions. The musculoskeletal sequelae of being underweight often include decreased muscle mass, decreased soft tissue mass, as well as a higher incidence of osteoporosis [5]. These factors are not inconsequential considerations for the orthopedic surgeon performing total hip replacement surgery, as previous studies have demonstrated higher rates of dislocations in underweight patients compared to normal weight individuals [5,17,18]. We believe this finding is likely due to these patients’ decreased muscle mass and soft tissue tension around the hip joint associated with their underweight status.
We recognize that the present study has certain limitations—most notably that it is a retrospective review, with all of the attendant limitations including reliance on the accuracy and completeness of hospital records within our electronic database. Another limitation is the relatively low number of underweight patients, representing 1.29% of our study population. While this incidence falls slightly below the most recent estimated national prevalence of 1.7% [6], it does represent a larger percentage of underweight patients than found within the first study reporting increased complications in this group where only 0.46% of their patients were underweight [5]. An additional limitation is that we did not specifically control for other comorbidities, such as diabetes, cardiovascular disease, or smoking. The present study does not claim that BMI is an independent risk factor for THA complications, and it is likely that patients with both high and low BMI have associated comorbidities that play a role in their complications. It is well understood that BMI has significant limitations as a predictor, and we simply wanted to see if there were increased complications in both high and low BMI patients that had not been previously reported. A larger dataset, preferably multicenter, would be required to appropriately control for comorbid conditions and assess the existence of an independent association.
As mentioned above, there are also certain limitations to BMI in and of itself. One of these limitations is that BMI may simply be a surrogate marker for nutritional status, as obese patients can often have paradoxical malnutrition. While BMI may represent an indirect measure of nutritional status, studies have shown that albumin may actually be a better predictor than BMI of outcomes after coronary artery bypass surgery [30]. Future studies are needed to examine a larger population of underweight and obese patients undergoing THA, specifically looking at nutritional status/indices and other metabolic factors that may also contribute to postoperative complications. Similarly, there is the inability of BMI to distinguish adiposity from lean mass [31]. BMI is a quick and easy indicator of excess adiposity; however, the accuracy varies according to the relative amounts of adiposity and lean mass [32,33]. Mehta et al. [34] recently showed how weight distribution is more strongly associated with infection risk than BMI in patients undergoing lumbar spinal fusion surgery. Future studies may use a more accurate assessment of true body mass and perhaps include screens for metabolic risk factors associated with obesity, such as metabolic syndrome. Indeed, metabolic syndrome and its relationship to total joint arthroplasty have started to gain attention [26,35]. Gonzales et al. [35] showed that metabolic syndrome was an independent risk factor for the development of major complications, nonroutine discharge, and increased hospital cost in patients undergoing total hip and knee arthroplasty. Likewise, Saucedo et al. [36] found a U-shaped trend relating underweight and obese patient populations to an increased cost associated with post-operative complications, reporting that low BMI was an independent risk factor for readmission within 90 days following THA, and that a high BMI was significant for readmission within 30 days following total knee arthroplasty surgery. These findings, along with those of the present study, provide further evidence that these 2 patient populations are at increased risk for postoperative complications; thus, representing a significant financial burden to the patient, hospital, and society as a whole. In today’s rapidly changing healthcare environment, hospitals and physicians face increasing pressure to decrease surgical and medical complications that lead to higher cost. By understanding how BMI may affect our outcomes, we can attempt to influence this potentially modifiable risk factor preoperatively to help reduce costs related to postoperative complications. CONCLUSIONS
This study further indicates the increased rate of medical complications for patients with both high and low BMI who undergo primary THA. Given the rising cost of healthcare, it is important to recognize the association between postoperative complications in both the obese and underweight patient populations. Future studies to better define the relationship between underweight patients and postoperative complications are needed, as this is a small, but not insignificant, subset of arthroplasty patients. REFERENCES
[1] Ogden C, Carroll M, Kit B, Flegal K (2012) Prevalence of Obesity in the United States 2009-2010. NCHS data brief, no 82. Hyattsville, MD: National Center for Health Statistics. 2012.
[2] Hohmander LS, Gerhardsson de Verdier M, Rollof J. Incidence of severe knee and hip osteoarthritis in relation to different measures of body mass: a population-based prospective cohort study. Ann Rheum Dis. 2009;68:490-6.
[3] Järvholm B, Lewold S, Malchau H, Vingård E. Age, bodyweight, smoking habits and the risk of severe osteoarthritis in the hip and knee in men. Eur J Epidemiol. 2005;20:537-42.
[4] Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89:780-5.
[5] Alfonso DT, Howell RD, Caceres G, Kozlowski P, DiCesare PE. Total hip arthroplasty in the underweight. J Arthroplasty. 2008;23:956-9.
[6] Fryar CD, Ogden CL. Prevalence of underweight among adults aged 20 years and over: United States, 1960-1962 through 2007-2010. Available at: http://www.cdc.gov/nchs/data/hestat/underweight_adult_07_10/underweight_adult_07_10.pdf
[7] Flegal KM, Graubard BI, Williamson DF, Gail MH. Excess deaths associated with underweight, overweight, and obesity. JAMA. 2005;293:1861-7.
[8] Ringback WG, Eliasson M, Rosen M. Underweight, overweight and obesity as risk factors for mortality and hospitalization. Scand J Public Health. 2008;36:169-76.
[9] World Health Organization. BMI Classification. http://apps.who.int/bmi/index.jsp?introPage=intro_3.html
[10] Luleiman LI, Orgeta G, Onguti S, Gonzalez DO, Tran DD, Onyike A, Turner PL, Fullum TM. Does BMI affect perioperative complications following total knee and hip arthroplasty? J Surg Res. 2012;174:7-11.
[11] Moran M, Walmsley P, Gray A, Brenkel IJ. Does body mass index affect the early outcome of primary total hip arthroplasty? J Arthroplasty. 2005;20:866-9.
[12] Jiganti JJ, Goldstein WM, Williams CS. A comparison of the perioperative morbidity in total joint arthroplasty in the obese and non-obese patient. Clin Orthop Relat Res. 1993;289: 175-9.
[13] Suleiman LI, Ortega G, Ong'uti SK, Gonzalez DO, Tran DD, Onyike A, Turner PL, Fullum TM. Does BMI affect perioperative complications following total knee and hip arthroplasty? J Surg Res. 2012;174:7-11.
[14] Namba RS, Paxton L, Fithian DC, Stone ML. Obesity and perioperative morbidity in total hip and total knee arthroplasty patients. J Arthroplasty. 2005;20:46-50.
[15] Jain NB, Guller U, Pietrobon R, Bond TK, Higgins LD. Comorbidities increase complication rates in patients having arthroplasty. Clin Orthop Relat Res. 2005;435:232-8.
[16] Chee JH, Teoh KH, Sabnis BM, Ballantyne JA, Brenkel IJ. Total hip replacement in morbidly obese patients with osteoarthritis. J Bone Joint Surg Br. 2010;92B:1066-71.
[17] Marks R. Body mass characteristics of hip osteoarthritis patients experiencing aseptic loosening, periprosthetic fractures, dislocation, and infections after total hip replacement. Clinicoecon Outcomes Res. 2009;1:7-16
[18] Zhang ZJ, Zhao XY, Kang Y, Zhang ZQ, Yang ZB, He AS, Fu M, Sheng PY, Liao WM. The influence of body mass index on life quality and clinical improvement after total hip arthroplasty. J Orthop Sci. 2012;17:219-25.
[19] Murgatroyd SE, Frampton CM, Wright MS. The effect of body mass index on outcome in total hip arthroplasty: early analysis from the New Zealand joint registry. J Arthroplasty. 2014;29:1884-8.
[20] Sabharwal S, Root MZ. Impact of obesity on orthopaedics. J Bone joint Surg Am. 2012;94:1045-52.
[21] Wagner BD, Grunwald GK, Rumsfeld JS, Hill JO, Ho PM, Wyatt HR, Shroyer AL. Relationship of body mass index with outcomes after coronary artery bypass graft surgery. Ann Thorac Surg. 2007;84:10-6.
[22] Atalan N, Fazlioqullan O, Kunt AT, Basaran C, Gurer O, Sitilci T, Akqun S, Arsan S. Effect of body mass index on early morbidity and mortality after isolated coronary artery bypass graft surgery. J Cardiothorac Vasc Anesth. 2012;26:813-7.
[23] Dowsey MM, Choong FM. Obesity is a major risk factor for prosthetic infection after primary hip arthroplasty. Clin Orthop Relat Res. 2008;466:153-8.
[24] Malinzak RA, Ritter MA, Berend ME, Meding JB, Olberding EM, Davis KE. Morbidly obese, diabetic, younger, and unilateral joint arthroplasty patients have elevated total joint arthroplasty infection rates. J Arthroplasty. 2009;24:84-8.
[25] Jamsen E, Nevalainen P, Eskelinen A, Huotari K, Kalliovalkama J, Moilanen T. Obesity, diabetes, and preoperative hyperglycemia as predictors of periprosthetic joint infection. J Bone Joint Surg Am. 2012;94:e101.
[26] Miller RS, Norris PR, Jenkins JM, Talbot TR, Starmer JM, Hutchison SA, Carr DS, Kleymeer CJ, Morris JA. Systems initiatives reduce healthcare-associated infections; a study of 22,928 device days in a single trauma unit. J Trauma. 2010;68:23-31.
[27] Knoll BM, Wright D, Ellingson L, Kraemer L, Patire R, Kuskowski MA, Johnson JR. Reduction of inappropriate urinary catheter use at a veterans affairs hospital through a multifaceted quality improvement project. Clin Infect Dis. 2011;52:1283-90.
[28] Patel AD, Albrizio M. Relationship of body mass index to early complications in knee replacement surgery. Arch Orthop Trauma Surg. 2008;128:5-9.
[29] Leahy, M. TKA improves function regardless of patient’s BMI. AAOS Now. October 2012.
[30] Bhamidipati CM, LaPar DJ, Mehta GS, Kern JA, Upchurch GR Jr, Kron IL, Ailawadi G. Albumin is a better predictor of outcomes than body mass index following coronary artery bypass grafting. Surgery. 2011;150:626-34.
[31] Ferguson DF, Busenlehner BJ, Rahm MD, Mehta SM, Song J, Davis ML, Sampson W, Chaput CD. The use of routine thoracoabdominal CT scans in the polytrauma patient to estimate obesity. Obesity. 2012;21:997-1003.
[32] Okorodudu DO, Jumean MF, Montori VM, Romero-Corral A, Somers VK, Erwin PJ, Lopez-Jimenez F. Diagnostic performance of body mass index to identify obesity as defined by body adiposity: a systematic review and meta-analysis. Int J Obes. 2010;34:791-9.
[33] Romero-Corral A, Somers VK, Sierra-Johnson J, Thomas RJ, Collazo-Clavell ML, Korinek J, Allison TG, Batsis JA, Sert-Kuniyoshi FH, Lopez-Jimenez F. Accuracy of body mass index in diagnosing obesity in the adult general population. Int J Obes (Lond) 2008;32:959-6.
[34] Mehta AI, Babu R, Karikari IO, Grunch B, Agarwal VJ, Owens TR, Friedman AH, Bagley CA, Gottfried ON. The distribution of body mass as a significant risk factor for lumbar spinal fusion postoperative infections. Spine. 2012;37: 1652-6.
[35] Gonzalez Della Valle AG, Chiu YL, Ma Y, Mazumdar M, Memtsoudis SG. The metabolic syndrome in patients undergoing knee and hip arthroplasty: trends and in-hospital outcomes in the United States. J Arthroplasty. 2012;27:1743-9.
[36] Saucedo JM, Marecek GS, Wanke TR, Lee J, Stulberg SD, Puri L. Understanding readmission after primary total hip and knee arthroplasty: who’s at risk? J Arthroplasty. 2014;29:256-60.