
Outcome of a Treatment Protocol for Severe Open and Unstable Dislocations of the Ankle
Massimo M. Morandi, MD, FACS¹; Jessica Faught, MD¹; Sebastiano Mangano, MD²
¹Department of Orthopaedic Surgery, Louisiana State University; Shreveport, LA, USA
²Presidio Ospedaliero Vittorio Emanuele di Gela; Gela, Catania, Italy
Corresponding Author:Massimo M. Morandi MD, FACS, Department of Orthopaedic Surgery, Louisiana State University, 1501 Kings Hwy, Shreveport, LA 71130; USA; mmoran@lsuhsc.edu
DOI: 10.18600/toj.020108
INTRODUCTION
Fracture-dislocation/open dislocations of the tibiotalar joint were first described by Dupuytren in 1819 [1]. These are complex injuries associated with high-energy trauma, largely as a result of a motor vehicle accident [2]. There is a high incidence of reported treatment complications, particularly deep infection. It is the impression of a number of trauma surgeons that the frequency of this group of injuries may be increasing [3]. This increase could be explained by improved resuscitation of the polytraumatized patient at the scene of the accident, improved patient transit times, and the increasing use of airbags and other safety precautions in motor vehicles. All of these factors contribute to an increased survival rate, enabling patients who would have died in previous years, now to be transported and treated expeditiously at a Level I Trauma Center where their orthopaedic injuries are promptly recognized and managed. This increase in cases is also due to a lack of safety measures in motor vehicles for the lower extremities. Ankle dislocations, with or without associated fractures, are a frequent sequela from these high-energy trauma, and commonly are open injuries. The management of these lesions is controversial and complications are common, leaving many patients with severely altered ankle functions and, thus, altered employment and recreation. We have developed a protocol for these unstable ankle dislocations and found that its institution has led to excellent outcomes, few complications, and the ability for most of our patients to return to work in their preinjury capacity. This standard treatment protocol has been developed to simplify the management of these complex injuries and has been implemented by the senior author for more 20 years. MATERIALS & METHODS
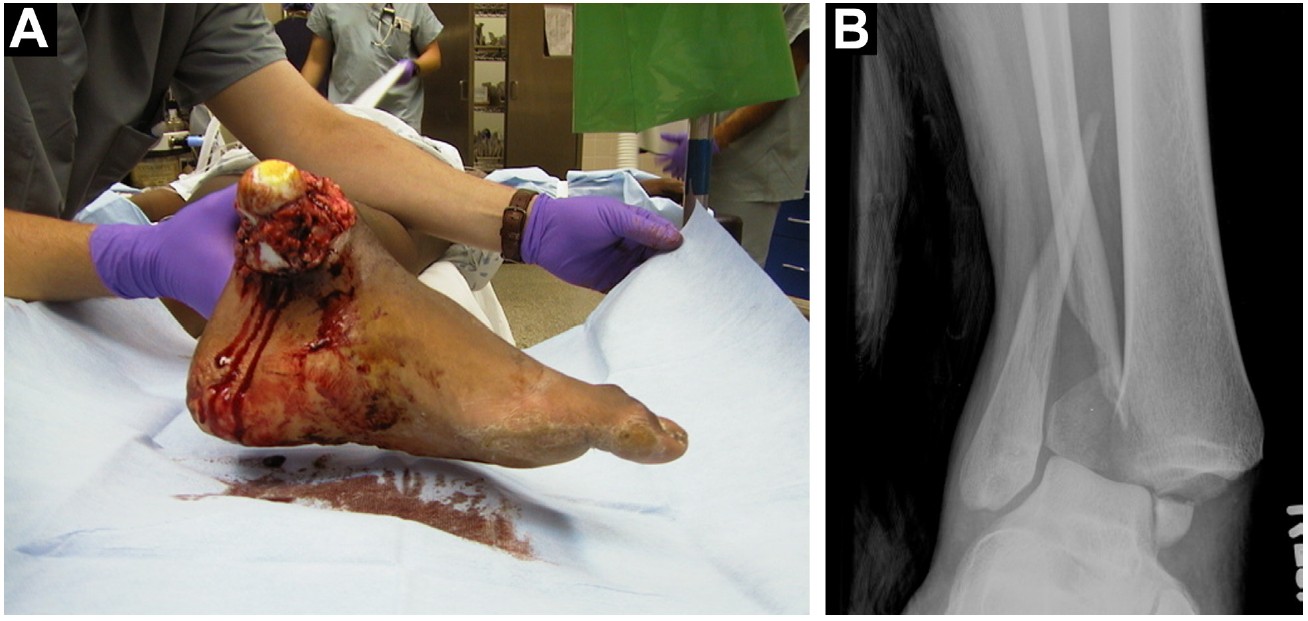
Our protocol consists of initial trauma room evaluation by the orthopaedic resident (Figure 1). The patient is assessed in the emergency room (ER) and the distal neurovascular status is established. The dislocations that were not grossly contaminated are reduced under intravenous analgesia and sedation and a padded trilaminar splint applied as temporary immobilization. Betadine dressings are placed over grossly contaminated open injuries that are splinted without reduction. The intravenous antibiotics (eg, ancef 2g, gentamicin 5mg/kg) and tetanus prophylaxis are administered before the patient leaves the ER. Grossly contaminated wounds also receive 4 million units of penicillin. The patients then are taken to the operating room (OR) emergently for irrigation, surgical exploration, and debridement, followed by skeletal stabilization.
Fracture-dislocation/open dislocations of the tibiotalar joint were first described by Dupuytren in 1819 [1]. These are complex injuries associated with high-energy trauma, largely as a result of a motor vehicle accident [2]. There is a high incidence of reported treatment complications, particularly deep infection. It is the impression of a number of trauma surgeons that the frequency of this group of injuries may be increasing [3]. This increase could be explained by improved resuscitation of the polytraumatized patient at the scene of the accident, improved patient transit times, and the increasing use of airbags and other safety precautions in motor vehicles. All of these factors contribute to an increased survival rate, enabling patients who would have died in previous years, now to be transported and treated expeditiously at a Level I Trauma Center where their orthopaedic injuries are promptly recognized and managed. This increase in cases is also due to a lack of safety measures in motor vehicles for the lower extremities. Ankle dislocations, with or without associated fractures, are a frequent sequela from these high-energy trauma, and commonly are open injuries. The management of these lesions is controversial and complications are common, leaving many patients with severely altered ankle functions and, thus, altered employment and recreation. We have developed a protocol for these unstable ankle dislocations and found that its institution has led to excellent outcomes, few complications, and the ability for most of our patients to return to work in their preinjury capacity. This standard treatment protocol has been developed to simplify the management of these complex injuries and has been implemented by the senior author for more 20 years. MATERIALS & METHODS
Our protocol consists of initial trauma room evaluation by the orthopaedic resident (Figure 1). The patient is assessed in the emergency room (ER) and the distal neurovascular status is established. The dislocations that were not grossly contaminated are reduced under intravenous analgesia and sedation and a padded trilaminar splint applied as temporary immobilization. Betadine dressings are placed over grossly contaminated open injuries that are splinted without reduction. The intravenous antibiotics (eg, ancef 2g, gentamicin 5mg/kg) and tetanus prophylaxis are administered before the patient leaves the ER. Grossly contaminated wounds also receive 4 million units of penicillin. The patients then are taken to the operating room (OR) emergently for irrigation, surgical exploration, and debridement, followed by skeletal stabilization.
In the OR (Figure 2), the patient is placed on a radiolucent table once anesthesia is induced, and a padded tourniquet is applied to the ipsilateral thigh. A bump is placed under the buttock to prevent external rotation, and the leg is then positioned over a long-bone foam to facilitate intraoperative radiography. For open injuries, the ankles are re-dislocated for inspection of the joint surface. Sometimes, gross debris (grass, soil, gravel) is removed before a formal skin preparation is performed. After draping the extremity, the open wound is irrigated with 9 liters of saline, using a pulsatile lavage system as the author's preferred irrigation method. All necrotic, devitalized, and severely contused tissue is debrided.
The ankle joint is grossly unstable and therefore the articular surfaces are easily visualized. Any damage to the articular cartilage is recorded, and the joint is washed out through the open wound which is usually located over the medial malleolus. In the case of minimal open injury, a surgical exploration with Z-incision of the soft tissue is performed to allow for a better investigation of the joint space.
Following irrigation and debridement, the surgeon changes his gloves and gown, the leg is re-draped, and the used instruments discarded. Internal fixation is then performed if a fracture is present and most frequently this involves the distal fibula. The fracture is exposed via a longitudinal incision taking care not to injure the superficial peroneal nerve. The fracture is frequently comminuted and anatomical reduction may be impossible. In this situation, it is important to restore fibula length and rotation, and a comparative mortise radiograph of the other side may be helpful. In the presence of major fracture comminution of a proximal fibular fracture and an unstable joint, we favor fixation with a 3.5 dynamic compression plate (Synthes; Paoli, PA, USA). Less severe, more distal fractures are secured with a one-third tubular plate with specially designed hook plates. After reduction and fixation of the fibular fracture, the integrity of the syndesmosis is assessed. A hook is placed around the fibula and an attempt is made to widen the syndesmosis and demonstrate tibiofibular diastasis while screening the syndesmosis on the image intensifier. If instability is demonstrated, the syndesmosis must be accurately reduced. We use a large Weber pointed reduction forceps (Synthes; Paoli, PA, USA) which is applied between an empty hole in the plate laterally and the cortex above the medial malleolus medially. The syndesmosis must be accurately reduced before insertion of a syndesmosis screw, as the screw is designed to hold the reduction and not provide compression. If the medial malleolus is fractured, the fragment is reduced and secured with two 4.0 mm cannulated, partially threaded cancellous screws (Synthes; Paoli, PA, USA). The deltoid ligament is not repaired if ruptured. All the open soft tissues injuries are again irrigated and the nonsurgical incisions are left open, if necessary. The temporary coverage of the soft tissue has been obtained with synthetic skin (Epigard®, Medisafe GmbH, Germany) or with vacuum-assisted devices.
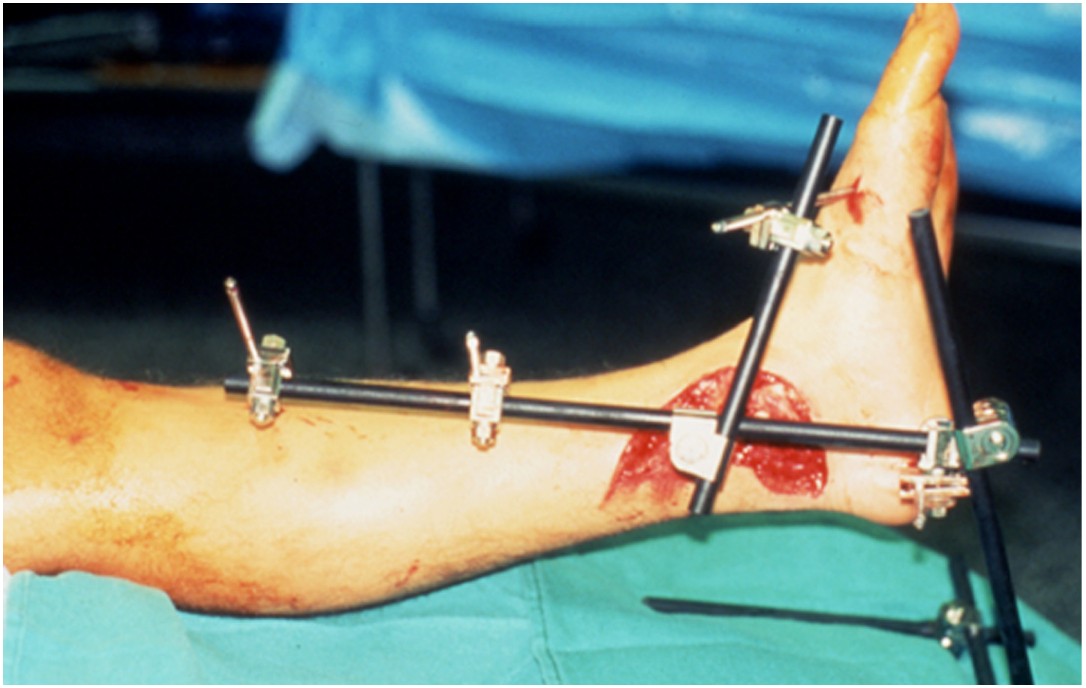
Once internal fixation of the ankle is complete, the foot and ankle are stabilized with an external fixator (Figure 3). Even in cases with fracture of the talus or pure dislocation, we span the reduced ankle joint, applying the ex-fix in the same manner. We have used 1 of 5 types of external fixators over time (Hex Fix; Smith & Nephew; Memphis, TN, USA; Large External Fixator; Synthes; Paoli, PA, USA; Jet-X External Fixator; Smith & Nephew; Memphis, TN, USA; Hoffmann External Fixator, Stryker; Kalamazoo, MI, USA; Dolphix, CiTiEffe, Bologna, Italy). Overall, we favor a simple, inexpensive, pre-packaged unilateral frame which ideally can be applied rapidly, even in the ER, without power tools.
The usual adopted configuration consists of 2 proximal pins that are inserted into the anteromedial aspect of the tibia. Another pin is placed in the calcaneus, and the bars of the fixator are attached to these pins. The calcaneal pin is inserted in a slightly valgus orientation so the ankle is placed into varus/supination once the fixator is tightened. Finally, the foot is dorsiflexed to 90 degrees, and another pin is inserted into the first metatarsal, using the metatarsal paddle and clamp as a drill guide. Care is taken to place the metatarsal pin so it does not obscure the ankle joint on the AP radiograph. The ankle is reduced, and all mountings are then tightened.
Once internal fixation of the ankle is complete, the foot and ankle are stabilized with an external fixator (Figure 3). Even in cases with fracture of the talus or pure dislocation, we span the reduced ankle joint, applying the ex-fix in the same manner. We have used 1 of 5 types of external fixators over time (Hex Fix; Smith & Nephew; Memphis, TN, USA; Large External Fixator; Synthes; Paoli, PA, USA; Jet-X External Fixator; Smith & Nephew; Memphis, TN, USA; Hoffmann External Fixator, Stryker; Kalamazoo, MI, USA; Dolphix, CiTiEffe, Bologna, Italy). Overall, we favor a simple, inexpensive, pre-packaged unilateral frame which ideally can be applied rapidly, even in the ER, without power tools.
The usual adopted configuration consists of 2 proximal pins that are inserted into the anteromedial aspect of the tibia. Another pin is placed in the calcaneus, and the bars of the fixator are attached to these pins. The calcaneal pin is inserted in a slightly valgus orientation so the ankle is placed into varus/supination once the fixator is tightened. Finally, the foot is dorsiflexed to 90 degrees, and another pin is inserted into the first metatarsal, using the metatarsal paddle and clamp as a drill guide. Care is taken to place the metatarsal pin so it does not obscure the ankle joint on the AP radiograph. The ankle is reduced, and all mountings are then tightened.

Soft-tissue swelling is common following these injuries, and the limb must be elevated postoperatively. Patients with open injuries return to the OR every other day for repeat irrigation and debridement until the soft tissues are ready for a secondary closure or surgical procedure by plastic surgery, usually 5 to 7 days later. Physical therapy consults are obtained immediately postop for nonweightbearing ambulation of the affected extremity; the patient will continue physical therapy for 6 weeks postop when the frame is removed. We prefer to remove the ex-fix in the operating room, although it can also be safely done in the office. The patients are then placed in a short-leg cast for 2 more weeks and allowed progressive weight bearing.
RESULTS
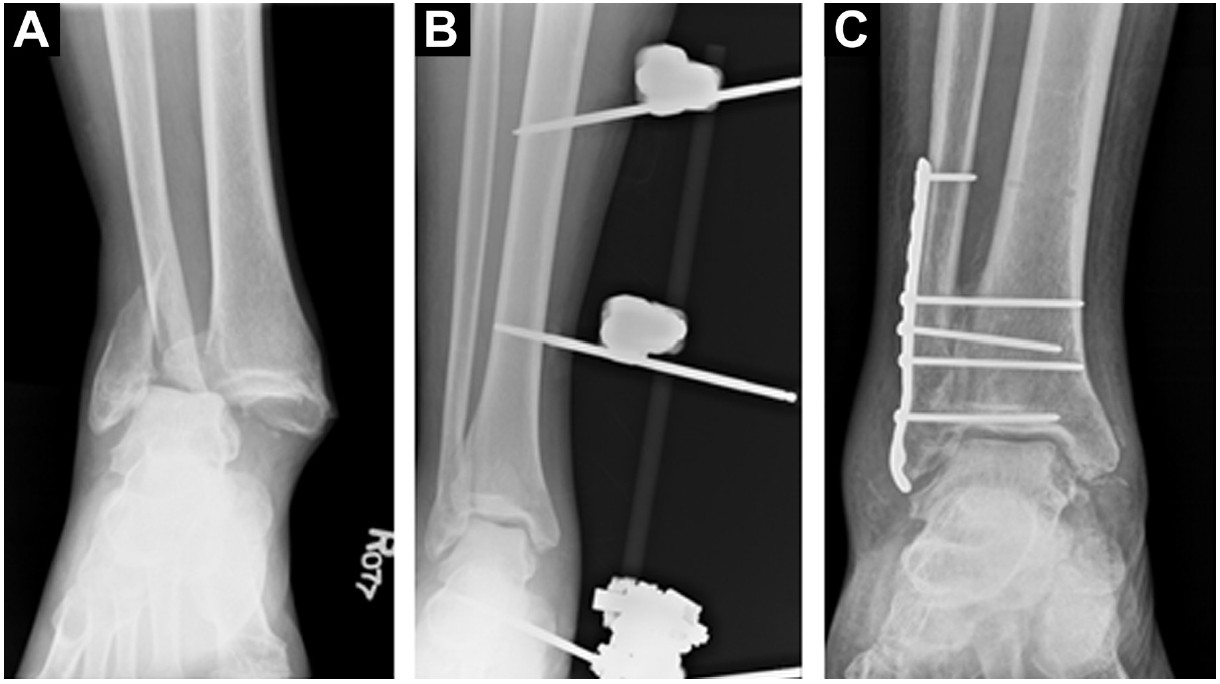
Our study evaluated 167 patients treated by this protocol. Follow-up was done at an average of 24.5 months (range 9 months to 5 years) (Figure 4). The open injuries included 35 grade II, 45 grade IIIA, and 113 grade IIIB. Since all these lesions involved the ankle joint, they were further classified as type IV open joint injuries, the most severe grade per Collins & Temple [4]. The average age of the patient was 35.7 years (range 21-62); 108 were men and 59 women. The mechanism of injury was an MVA in 108, a fall in 58, and timber fall in one patient. Alcohol intoxication was involved in more than 50% of the cases. All patients were treated by 1 surgeon. Only injuries involving the tibiotalar joint were included in this study. Any injury with a concomitant pilon fracture was excluded.
Our study evaluated 167 patients treated by this protocol. Follow-up was done at an average of 24.5 months (range 9 months to 5 years) (Figure 4). The open injuries included 35 grade II, 45 grade IIIA, and 113 grade IIIB. Since all these lesions involved the ankle joint, they were further classified as type IV open joint injuries, the most severe grade per Collins & Temple [4]. The average age of the patient was 35.7 years (range 21-62); 108 were men and 59 women. The mechanism of injury was an MVA in 108, a fall in 58, and timber fall in one patient. Alcohol intoxication was involved in more than 50% of the cases. All patients were treated by 1 surgeon. Only injuries involving the tibiotalar joint were included in this study. Any injury with a concomitant pilon fracture was excluded.
Outcome of treatment was evaluated using a combination of a patient questionnaire, subjective functional examinations at follow-up visits, and radiographic analysis of postreduction films by a musculoskeletal radiologist. The patient questionnaire was based on the original questionnaire by Sanders et al. [5]. It consisted of 11 questions asking the patient about their feelings regarding how severe they considered their injury, how successful they felt their treatment had been, and what type of activities they were able to resume. One hundred twenty-three of 167 patients believed that they were going to lose their leg at the time of the injury. That same number subsequently reported that their treatment was relatively uncomplicated. The average number of surgical procedures was 4.2 (range 2-8), while the range of hospitalization was 5-21 days. Pain continued to be the greatest complaint at last follow-up. Although 165 patients reported occasional pain, most discomfort was with extended periods of activity. Two patient developed severe pain and debilitating posttraumatic arthritis and required an ankle fusion. Of the 167 patients, 61 were able to return to work with only 43 patients in an altered capacity. As an aside, all those not able to return to work were receiving workman’s compensation for their injury. No avascular necrosis of the talus or tibia resulted. Two patients with large infected soft-tissue defects requested to avoid further debridements after their fourth subsequent surgical procedure and elected a below-knee amputation.
Superficial pin site irritation and superficial infection requiring frequent pin care were present at 1 time or another during the treatment period, with no difference noted in any particular fixator. Forty-two pins became loose, particularly in the calcaneus and the first metatarsal pins, with no difference in titanium or stainless steel fiches. The frame got loose in 17 cases at 1 or more of the clamps. No specific manufacturer was responsible. Plastic surgery with a vascularized free flap was implemented in 30 cases. There was a significant difference in plastic surgeon experience and procedure preference, but it did not adversely affect the results. The use of a free vascularized muscular flap appears to be a very appropriate solution in the case of severe soft-tissue damage. The use of vacuum-assisted devices did not seem to have the same temporary benefits as the Epigard®, especially in senior patients or patients with altered fluid retention.
DISCUSSION
Fracture-dislocations of the ankle are severe injuries associated with significant soft-tissue and bone damage [4]. We have focused our attention on open injuries involving the ankle joint treated and followed by the same surgeon. All cases had gross capsular disruption with instability associated with soft-tissue contamination.
The immediate aggressive debridement and stabilization of open ankle injuries, particularly grade IIIB injuries, is paramount. Early series of open-ankle fractures treated by ORIF had disturbingly high rates of infection. More recent studies, however, have reported lower infection rates after early external fixation. The reduction in infection is attributed to improved surgical techniques and attention to soft-tissue handling. Also, in cases of open injuries, the thorough, repeated irrigation and debridement with either delayed wound closure or early soft-tissue coverage combined with strict adherence to AO/ASIF principles have improved the overall results [2,3,6,7].
There have been a number of experimental and clinical studies on the syndesmosis which have increased our understanding of the syndesmotic injury and, in turn, may lead to improved functional results [8-10]. Fracture-dislocations represent severe ankle injuries, and when the syndesmosis is disrupted, the instability is even more severe. We therefore recommend accurate reduction of a tibiofibular diastasis before fixation with a syndesmosis screw. A large Weber reduction forceps is used and the reduction is carefully assessed radiographically before screw insertion.
It is the practice of most surgeons to put the majority, if not all, of their operatively treated ankle fractures into a cast for 2-6 weeks after fixation. Clearly, cast immobilization of severe ankle fracture-dislocations after internal fixation would cause numerous problems because a high incidence of open injuries have associated soft-tissue swelling, blistering, and edema. External fixation simplifies soft-tissue management by providing excellent wound access and is less cumbersome than the traditional cast. Previous literature has supported the efficacy and safety of spanning ankle external fixators for severe ankle trauma [10-12]. The secure immobilization ensures optimal capsular and ligamentous healing as well as further stabilization after bone dislocation or fracture fixation. There is no need for constrictive padding or bandages and wounds can be easily monitored for signs of infection. Plastic surgery is facilitated by the soft-tissue stability the fixator provides for vascularized free flaps and skin grafts. We have selected a very simple frame configuration which can be rapidly constructed and applied to the injured extremity. The average time of frame application in our series of cases was around 30 minutes. We feel it is important when applying an external fixator to the tibia that care is taken to avoid an equinus deformity at the ankle. Despite the external fixator’s ease of application, care must be taken when inserting the medial calcaneal pin to avoid the medial calcaneal and the lateral plantar nerves [13].
Our treatment protocol was designed to offer the surgeon a relatively quick, safe, and reliable way to address severely unstable ankle dislocations, while providing ease of access for soft-tissue management and ease of care for the patient. Gustilo and Anderson [14] noted that the most important prognostic factor in open fractures is the amount of energy absorbed to create the soft-tissue injury.
Our study shows that internal fixation with adjuvant external fixation is a viable option for even high-grade open fractures. This combination was designed to obtain anatomic restoration and stabilization of the ankle joint as an aid to manage the soft tissues, since early fracture stabilization maximizes the ability of the soft tissues to resist infection and to heal [15].
By using an external fixator as a supplement to internal fixation, we found we provided an ideal environment for soft-tissue healing and, therefore, an ideal environment for recovery [5]. Success can be defined in many terms, mainly by salvage of an extremity, patient satisfaction, and good functional use of the extremity. We found that this treatment protocol can be successful, with the majority of the patients able to return to their pre-injury social capacity. REFERENCES
[1] Dupuytren G. Mémoire sur la fracture de l’extrémité inférieure du péroné, les luxations et les accidents qui en sont la suite. In: Annuaire Médico-Chirurgical des Hôpitaux et Hospices de Paris. Paris, 1819.
[2] Bray TJ, Endicott M, Capra SE. Treatment of open ankle fractures. Immediate internal fixation versus closed immobilization and delayed fixation. Clin Orthop Relat Res. 1989;240:47-52.
[3] Burgess AR, Dischinger PC, O'Quinn TD, Schmidhauser CB. Lower extremity injuries in drivers of airbag-equipped automobiles: clinical and crash reconstruction correlations. J Trauma. 1995;38(4):509-16.
[4] Collins, DN, Temple, SD. Open joint injuries: classification and treatment. Clin Orthop Relat Res. 1980;243:48-56.
[5] Sanders, R, Pappas, J, Mast, J, Helfet, D. The salvage of open grade III ankle and talar fractures. J Orthop Trauma. 1992;6:201-8.
[6] Chapman MW, Mahoney M. The role of early internal fixation in the management of open fractures. Clin Orthop Relat Res. 1979;138:120-31.
[7] Johnson EE, Davlin LB. Open ankle fractures. The indications for immediate open reduction and internal fixation. Clin Orthop Relat Res. 1993;292:118-27.
[8] Mosheiff R, Liebergall M, Marguilies JY, Peyser A. London E, Segal D: Technical complication of the tibiofibular syndesmotic screw. J Foot Ankle Surg. 32:462, 1993.
[9] Chissell HR1, Jones J. The influence of a diastasis screw on the outcome of Weber type-C ankle fractures. J Bone Joint Surg Br. 1995;77(3):435-8.
[10] Anglen JO, Aleto T. Temporary transarticular external fixation of the knee and ankle. J Orthop Trauma. 1998;12(6):431-4.
[11] Patterson, MJ, Cole, JD. Two-staged delayed open reduction and internal fixation of severe pilon fractures. J Ortho Trauma. 1999;13(2):85-91.
[12] Rammelt S, Endres T, Grass R, Zwipp H. The role of external fixation in acute ankle trauma. Foot Ankle Clin. 2004;9(3):455-74.
[13] Casey D, McConnell T, Parekh S, Tornetta P. Percutaneous pin placement in the medial calcaneus: is anywhere safe? J Orthop Trauma. 2002;16(1):26-9.
[14] Gustilo RB, Anderson JT. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: retrospective and prospective analyses. J Bone Joint Surg Am. 1976;58(4):453-8.
[15] Pearce MF, Iero JJ, Morandi M. Severe fractures dislocations of the ankle joint: a management protocol. J Orthop Tech. 1995;3:164-8.
Fracture-dislocations of the ankle are severe injuries associated with significant soft-tissue and bone damage [4]. We have focused our attention on open injuries involving the ankle joint treated and followed by the same surgeon. All cases had gross capsular disruption with instability associated with soft-tissue contamination.
The immediate aggressive debridement and stabilization of open ankle injuries, particularly grade IIIB injuries, is paramount. Early series of open-ankle fractures treated by ORIF had disturbingly high rates of infection. More recent studies, however, have reported lower infection rates after early external fixation. The reduction in infection is attributed to improved surgical techniques and attention to soft-tissue handling. Also, in cases of open injuries, the thorough, repeated irrigation and debridement with either delayed wound closure or early soft-tissue coverage combined with strict adherence to AO/ASIF principles have improved the overall results [2,3,6,7].
There have been a number of experimental and clinical studies on the syndesmosis which have increased our understanding of the syndesmotic injury and, in turn, may lead to improved functional results [8-10]. Fracture-dislocations represent severe ankle injuries, and when the syndesmosis is disrupted, the instability is even more severe. We therefore recommend accurate reduction of a tibiofibular diastasis before fixation with a syndesmosis screw. A large Weber reduction forceps is used and the reduction is carefully assessed radiographically before screw insertion.
It is the practice of most surgeons to put the majority, if not all, of their operatively treated ankle fractures into a cast for 2-6 weeks after fixation. Clearly, cast immobilization of severe ankle fracture-dislocations after internal fixation would cause numerous problems because a high incidence of open injuries have associated soft-tissue swelling, blistering, and edema. External fixation simplifies soft-tissue management by providing excellent wound access and is less cumbersome than the traditional cast. Previous literature has supported the efficacy and safety of spanning ankle external fixators for severe ankle trauma [10-12]. The secure immobilization ensures optimal capsular and ligamentous healing as well as further stabilization after bone dislocation or fracture fixation. There is no need for constrictive padding or bandages and wounds can be easily monitored for signs of infection. Plastic surgery is facilitated by the soft-tissue stability the fixator provides for vascularized free flaps and skin grafts. We have selected a very simple frame configuration which can be rapidly constructed and applied to the injured extremity. The average time of frame application in our series of cases was around 30 minutes. We feel it is important when applying an external fixator to the tibia that care is taken to avoid an equinus deformity at the ankle. Despite the external fixator’s ease of application, care must be taken when inserting the medial calcaneal pin to avoid the medial calcaneal and the lateral plantar nerves [13].
Our treatment protocol was designed to offer the surgeon a relatively quick, safe, and reliable way to address severely unstable ankle dislocations, while providing ease of access for soft-tissue management and ease of care for the patient. Gustilo and Anderson [14] noted that the most important prognostic factor in open fractures is the amount of energy absorbed to create the soft-tissue injury.
Our study shows that internal fixation with adjuvant external fixation is a viable option for even high-grade open fractures. This combination was designed to obtain anatomic restoration and stabilization of the ankle joint as an aid to manage the soft tissues, since early fracture stabilization maximizes the ability of the soft tissues to resist infection and to heal [15].
By using an external fixator as a supplement to internal fixation, we found we provided an ideal environment for soft-tissue healing and, therefore, an ideal environment for recovery [5]. Success can be defined in many terms, mainly by salvage of an extremity, patient satisfaction, and good functional use of the extremity. We found that this treatment protocol can be successful, with the majority of the patients able to return to their pre-injury social capacity. REFERENCES
[1] Dupuytren G. Mémoire sur la fracture de l’extrémité inférieure du péroné, les luxations et les accidents qui en sont la suite. In: Annuaire Médico-Chirurgical des Hôpitaux et Hospices de Paris. Paris, 1819.
[2] Bray TJ, Endicott M, Capra SE. Treatment of open ankle fractures. Immediate internal fixation versus closed immobilization and delayed fixation. Clin Orthop Relat Res. 1989;240:47-52.
[3] Burgess AR, Dischinger PC, O'Quinn TD, Schmidhauser CB. Lower extremity injuries in drivers of airbag-equipped automobiles: clinical and crash reconstruction correlations. J Trauma. 1995;38(4):509-16.
[4] Collins, DN, Temple, SD. Open joint injuries: classification and treatment. Clin Orthop Relat Res. 1980;243:48-56.
[5] Sanders, R, Pappas, J, Mast, J, Helfet, D. The salvage of open grade III ankle and talar fractures. J Orthop Trauma. 1992;6:201-8.
[6] Chapman MW, Mahoney M. The role of early internal fixation in the management of open fractures. Clin Orthop Relat Res. 1979;138:120-31.
[7] Johnson EE, Davlin LB. Open ankle fractures. The indications for immediate open reduction and internal fixation. Clin Orthop Relat Res. 1993;292:118-27.
[8] Mosheiff R, Liebergall M, Marguilies JY, Peyser A. London E, Segal D: Technical complication of the tibiofibular syndesmotic screw. J Foot Ankle Surg. 32:462, 1993.
[9] Chissell HR1, Jones J. The influence of a diastasis screw on the outcome of Weber type-C ankle fractures. J Bone Joint Surg Br. 1995;77(3):435-8.
[10] Anglen JO, Aleto T. Temporary transarticular external fixation of the knee and ankle. J Orthop Trauma. 1998;12(6):431-4.
[11] Patterson, MJ, Cole, JD. Two-staged delayed open reduction and internal fixation of severe pilon fractures. J Ortho Trauma. 1999;13(2):85-91.
[12] Rammelt S, Endres T, Grass R, Zwipp H. The role of external fixation in acute ankle trauma. Foot Ankle Clin. 2004;9(3):455-74.
[13] Casey D, McConnell T, Parekh S, Tornetta P. Percutaneous pin placement in the medial calcaneus: is anywhere safe? J Orthop Trauma. 2002;16(1):26-9.
[14] Gustilo RB, Anderson JT. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: retrospective and prospective analyses. J Bone Joint Surg Am. 1976;58(4):453-8.
[15] Pearce MF, Iero JJ, Morandi M. Severe fractures dislocations of the ankle joint: a management protocol. J Orthop Tech. 1995;3:164-8.