
Evaluation of Negative Pressure Wound Therapy versus Dermabond Closure Over Orthopedic Incisions in the Hip and Knee
Craig Winkler, MD; Blake Clifton, MD; Adam Wooldridge, MD, MPH; Greg Anderson, MD, MBA; Greg Walker, MD; George Brindley, MD
Department of Orthopedic Surgery & Rehabilitation, Texas Tech University Health Sciences Center; Lubbock, TX, USA
Corresponding Author:Craig Winkler, MD, Department of Orthopaedics and Rehabilitation, Texas Tech University Health Sciences Center, 3601 4th Street, MS 9436, Lubbock, TX 79430, USA; craig.winkler@ttuhsc.edu
DOI: 10.18600/toj.020111
INTRODUCTION
For many years, joint reconstruction has been a very successful way of addressing degenerative joint disease. More than 1 million total hip and knee arthroplasties are done each year in the United States. It is estimated that this number will increase to over 4 million by the year 2030 [1].
Despite the benefits of total joint arthroplasty, there are several complications that can be devastating for the patient and difficult for the surgeon to treat. Many different precautions have been developed to reduce the risk of periopertive joint infection. Antibiotics, sterile technique, irrigation, and many other intraoperative and perioperative precautions are commonly used to ensure a successful outcome while minimizing the risk for infection. Surgical-incision closure is not only important to maintain the structural integrity of the incision, but also helps to minimize postoperative infections [2-5].
There are many different methods to close a surgical incision after an orthopaedic procedure [6]. Some methods have been shown to reduce risk of postoperative infection and have grown in favor over the last several years, including the use of 2-octylcyanoacrylate (OCA, Dermabond, Johnson & Johnson; New Brunswick, NJ). Dermabond (DB) provides a watertight barrier over a surgical incision limiting infection risk as well as maintaining structural integrity under tension, similar to, or better than, staples [5,7,8]. Quinn et al. [9] showed through an animal model that contaminated wounds closed with sutures had higher infection rates compared to an adhesive, demonstrating the benefit of DB over traditional sutures as a barrier to bacterial infection.
While an occlusive closure works well as a barrier to bacteria, it may also contribute to seroma formation and wound complications as fluid is unable to drain from tissue below the wound. This restriction can lead to unfavorable outcomes including wound infections, wound dehiscence, and a return to the operating room. Some have suggested that it may also cause a foreign body reaction when used in some individuals [10].
Negative pressure wound therapy (NPWT) has been used over orthopaedic incisions with a significant decrease in the size of the seroma compared with those treated without NPWT [11]. Many other studies in recent years have shown improved wound healing with the use of NPWT in both animal and human study models [3,4,11-15].
The objective of this study was to evaluate the difference between these 2 treatment methods (DB vs NPWT) for postoperative wound closure and subsequent wound complications. This retrospective review is, to our knowledge, the only study that directly compares postoperative surgical-incision infection risk after knee and hip arthroplasty between these 2 closure methods. MATERIALS & METHODS
Study Design
After receiving Institutional Review Board approval, a retrospective review of all patients that underwent total knee arthroplasty (TKA), unicompartmental knee arthroplasty (UKA), total hip arthroplasty (THA), and hip hemiarthroplasty was done to evaluate the outcomes of wound healing in a patient population with 2 distinct methods of wound closure and management following the above stated surgical procedures. All procedures we reviewed were performed at a single institution (University Medical Center; Lubbock, TX) and by a single surgeon (GWB) over a nearly 2-year period from August 2010 to June 2012.
The study identified 422 patients who underwent either TKA, UKA, revision TKA, THA, revision THA, or hip hemiarthroplasty. In addition to patient demographics, data was collected on wound-closure method, body mass index (BMI), tobacco use, comorbidities, and whether the procedure was necessary due to trauma or done on an elective basis. The primary outcome measure was wound complications and was defined as either uncomplicated (wound healing without dehiscence or infection), wound healing complicated by partial or full dehiscence of the wound without documented infection or need for any further procedures or antibiotic therapy, or partial or complete wound dehiscence with or without infection requiring a return trip to the operating room for surgical treatment of the wound. All patient records were reviewed until the wound was documented as completely healed in the postoperative clinic follow-up visits. If the patient had a previous arthroplasty or hemiarthroplasty, this was documented as well as any history of surgical site infection. All of these factors were examined as potential contributing factors to poor wound healing and further complications.
For the first year of the study, all patients’ surgical incisions were closed with Dermabond over a continuous 3.0 subcuticular absorbable suture (Monocryl, Johnson & Johnson; New Brunswick, NJ). The surgeon (GWB) noticed an increased number of surgical incisions that were draining several days out from surgery, and he also thought that he had a higher incidence of postoperative infections compared to previous years. It was under these circumstances that the surgeon’s preference changed to begin closing his surgical incision with nylon suture followed by an incisional wound VAC (Negative Pressure Wound Therapy System, KCI; San Antonio, TX). During the following 10 months that we reviewed, all surgical incisions in the above stated patient population were closed with nylon in the skin followed by an incisional wound VAC over the incision that was left in place until the patient was discharged from the hospital.
Patients’ incisional wound VAC dressings were removed when they were discharged from the hospital, and soft dressings were placed over the incisions. Patients in both groups were seen back in clinic 2 weeks after surgery and then again 6 weeks after surgery unless clinical concern warranted closer follow up. The primary surgeon described in detail the condition of the surgical wound, whether or not there was erythema, drainage, dehiscence, or gross purulence present. We based our findings on his descriptions of the wounds postoperatively. There were a total of 217 patients in the DB group over the first 12 months, and 205 patients in the NPWT group over the following 10 months.
In the DB group, patients’ incisions were evaluated daily while they were in the hospital, beginning postoperative day 2 after the initial operating room dressings were taken down. Any wound complications during their hospital stay were documented. On the day of discharge, a clean dressing was placed over the wound by the nursing staff with instructions to keep their dressing on, clean and dry, until follow-up in clinic. Patients in the NPWT group had their incisional wound VAC on throughout their stay in the hospital. On the day of discharge, the NPWT was discontinued and a clean dressing was placed over the wound with instructions to keep their dressing on, clean and dry, until follow-up in clinic. Evaluation of wound healing was performed for both groups at the clinic follow-up visit at 2 and 6 weeks postoperatively unless clinical concern warranted more frequent follow-up.
The patients with no drainage from their incisions in both groups were classified into group 1. Incisions in both groups with any amount of drainage postoperatively were classified into group 2. If there was drainage from the incision with partial or full dehiscence of the wound that required a return to the operating room, these patients were classified into group 3.
Within the study group, 11 patients were excluded due to lack of follow-up, death prior to wound healing, and/or incomplete medical records.
For many years, joint reconstruction has been a very successful way of addressing degenerative joint disease. More than 1 million total hip and knee arthroplasties are done each year in the United States. It is estimated that this number will increase to over 4 million by the year 2030 [1].
Despite the benefits of total joint arthroplasty, there are several complications that can be devastating for the patient and difficult for the surgeon to treat. Many different precautions have been developed to reduce the risk of periopertive joint infection. Antibiotics, sterile technique, irrigation, and many other intraoperative and perioperative precautions are commonly used to ensure a successful outcome while minimizing the risk for infection. Surgical-incision closure is not only important to maintain the structural integrity of the incision, but also helps to minimize postoperative infections [2-5].
There are many different methods to close a surgical incision after an orthopaedic procedure [6]. Some methods have been shown to reduce risk of postoperative infection and have grown in favor over the last several years, including the use of 2-octylcyanoacrylate (OCA, Dermabond, Johnson & Johnson; New Brunswick, NJ). Dermabond (DB) provides a watertight barrier over a surgical incision limiting infection risk as well as maintaining structural integrity under tension, similar to, or better than, staples [5,7,8]. Quinn et al. [9] showed through an animal model that contaminated wounds closed with sutures had higher infection rates compared to an adhesive, demonstrating the benefit of DB over traditional sutures as a barrier to bacterial infection.
While an occlusive closure works well as a barrier to bacteria, it may also contribute to seroma formation and wound complications as fluid is unable to drain from tissue below the wound. This restriction can lead to unfavorable outcomes including wound infections, wound dehiscence, and a return to the operating room. Some have suggested that it may also cause a foreign body reaction when used in some individuals [10].
Negative pressure wound therapy (NPWT) has been used over orthopaedic incisions with a significant decrease in the size of the seroma compared with those treated without NPWT [11]. Many other studies in recent years have shown improved wound healing with the use of NPWT in both animal and human study models [3,4,11-15].
The objective of this study was to evaluate the difference between these 2 treatment methods (DB vs NPWT) for postoperative wound closure and subsequent wound complications. This retrospective review is, to our knowledge, the only study that directly compares postoperative surgical-incision infection risk after knee and hip arthroplasty between these 2 closure methods. MATERIALS & METHODS
Study Design
After receiving Institutional Review Board approval, a retrospective review of all patients that underwent total knee arthroplasty (TKA), unicompartmental knee arthroplasty (UKA), total hip arthroplasty (THA), and hip hemiarthroplasty was done to evaluate the outcomes of wound healing in a patient population with 2 distinct methods of wound closure and management following the above stated surgical procedures. All procedures we reviewed were performed at a single institution (University Medical Center; Lubbock, TX) and by a single surgeon (GWB) over a nearly 2-year period from August 2010 to June 2012.
The study identified 422 patients who underwent either TKA, UKA, revision TKA, THA, revision THA, or hip hemiarthroplasty. In addition to patient demographics, data was collected on wound-closure method, body mass index (BMI), tobacco use, comorbidities, and whether the procedure was necessary due to trauma or done on an elective basis. The primary outcome measure was wound complications and was defined as either uncomplicated (wound healing without dehiscence or infection), wound healing complicated by partial or full dehiscence of the wound without documented infection or need for any further procedures or antibiotic therapy, or partial or complete wound dehiscence with or without infection requiring a return trip to the operating room for surgical treatment of the wound. All patient records were reviewed until the wound was documented as completely healed in the postoperative clinic follow-up visits. If the patient had a previous arthroplasty or hemiarthroplasty, this was documented as well as any history of surgical site infection. All of these factors were examined as potential contributing factors to poor wound healing and further complications.
For the first year of the study, all patients’ surgical incisions were closed with Dermabond over a continuous 3.0 subcuticular absorbable suture (Monocryl, Johnson & Johnson; New Brunswick, NJ). The surgeon (GWB) noticed an increased number of surgical incisions that were draining several days out from surgery, and he also thought that he had a higher incidence of postoperative infections compared to previous years. It was under these circumstances that the surgeon’s preference changed to begin closing his surgical incision with nylon suture followed by an incisional wound VAC (Negative Pressure Wound Therapy System, KCI; San Antonio, TX). During the following 10 months that we reviewed, all surgical incisions in the above stated patient population were closed with nylon in the skin followed by an incisional wound VAC over the incision that was left in place until the patient was discharged from the hospital.
Patients’ incisional wound VAC dressings were removed when they were discharged from the hospital, and soft dressings were placed over the incisions. Patients in both groups were seen back in clinic 2 weeks after surgery and then again 6 weeks after surgery unless clinical concern warranted closer follow up. The primary surgeon described in detail the condition of the surgical wound, whether or not there was erythema, drainage, dehiscence, or gross purulence present. We based our findings on his descriptions of the wounds postoperatively. There were a total of 217 patients in the DB group over the first 12 months, and 205 patients in the NPWT group over the following 10 months.
In the DB group, patients’ incisions were evaluated daily while they were in the hospital, beginning postoperative day 2 after the initial operating room dressings were taken down. Any wound complications during their hospital stay were documented. On the day of discharge, a clean dressing was placed over the wound by the nursing staff with instructions to keep their dressing on, clean and dry, until follow-up in clinic. Patients in the NPWT group had their incisional wound VAC on throughout their stay in the hospital. On the day of discharge, the NPWT was discontinued and a clean dressing was placed over the wound with instructions to keep their dressing on, clean and dry, until follow-up in clinic. Evaluation of wound healing was performed for both groups at the clinic follow-up visit at 2 and 6 weeks postoperatively unless clinical concern warranted more frequent follow-up.
The patients with no drainage from their incisions in both groups were classified into group 1. Incisions in both groups with any amount of drainage postoperatively were classified into group 2. If there was drainage from the incision with partial or full dehiscence of the wound that required a return to the operating room, these patients were classified into group 3.
Within the study group, 11 patients were excluded due to lack of follow-up, death prior to wound healing, and/or incomplete medical records.
Statistical Analysis
Demographic and clinical data were summarized and compared using Student t-test, Chi-square, or Fisher’s exact test. Descriptive summaries of continuous variables were presented in means, and discrete variables in frequencies and percentages. Odds ratios and 95% confidence intervals for postoperative wound healing were estimated using univariable and multivariable logistic regression models (Hosmer and Lemeshow). Variables included in the final model were selected on the basis of statistically significant univariable models, historically confirmed confounders, and stepwise hierarchical forward selection. Variables with p<0.05 were included in the model. Analyses were conducted with Stata version 12 software (StataCorp; College Station, TX). All statistical tests were 2-sided and a p value less than 0.05 indicated statistical significance. RESULTS
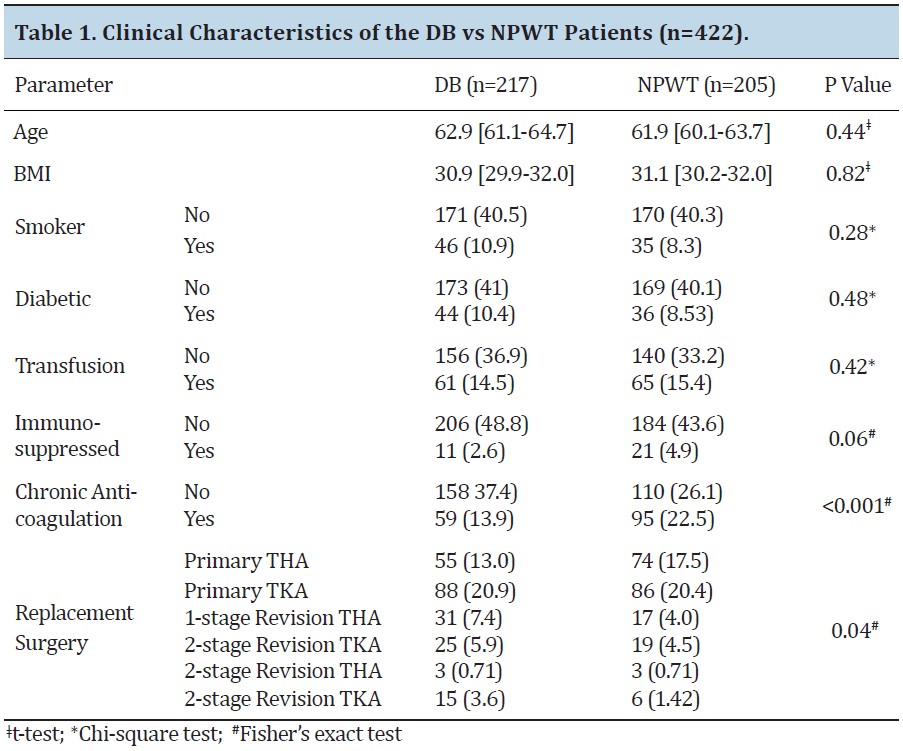
Of the 422 cases reviewed, 129 (30.6%) were primary THA, 174 (41.2%) were primary TKA; 48 (11.4%) were 1-stage revision THA; 44 (10.4%) were 1-stage revision TKA; 6 (1.4%) were 2-stage revision THA; and 21 (5.0%) were 2 stage revision TKA. DB was used to close skin in 217 cases and NPWT was used in 205 cases. The distribution of the variables of age, BMI, tobacco use, and diabetes mellitus were equally distributed among the DB and NPWT groups (Table 1).
Demographic and clinical data were summarized and compared using Student t-test, Chi-square, or Fisher’s exact test. Descriptive summaries of continuous variables were presented in means, and discrete variables in frequencies and percentages. Odds ratios and 95% confidence intervals for postoperative wound healing were estimated using univariable and multivariable logistic regression models (Hosmer and Lemeshow). Variables included in the final model were selected on the basis of statistically significant univariable models, historically confirmed confounders, and stepwise hierarchical forward selection. Variables with p<0.05 were included in the model. Analyses were conducted with Stata version 12 software (StataCorp; College Station, TX). All statistical tests were 2-sided and a p value less than 0.05 indicated statistical significance. RESULTS
Of the 422 cases reviewed, 129 (30.6%) were primary THA, 174 (41.2%) were primary TKA; 48 (11.4%) were 1-stage revision THA; 44 (10.4%) were 1-stage revision TKA; 6 (1.4%) were 2-stage revision THA; and 21 (5.0%) were 2 stage revision TKA. DB was used to close skin in 217 cases and NPWT was used in 205 cases. The distribution of the variables of age, BMI, tobacco use, and diabetes mellitus were equally distributed among the DB and NPWT groups (Table 1).
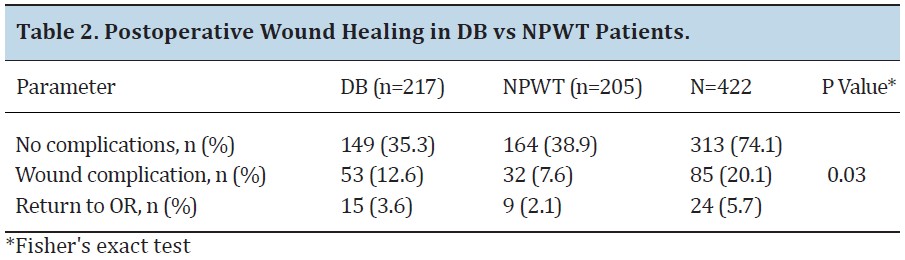
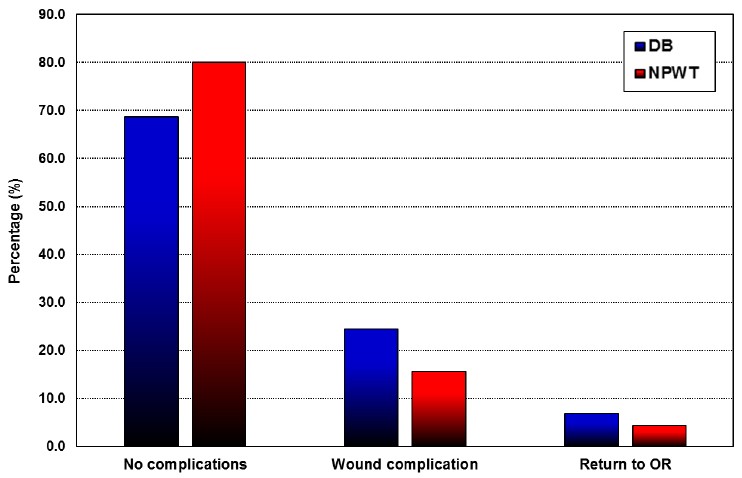
Most patients (313, 74.1%) were in Group 1 with no postoperative wound healing complications. Group 2 patients (85, 20.1%) had postoperative wound complications without a return to the operating room, and Group 3 patients (24, 5.7%) had wound complications that required a repeat operation. The NPWT group had significantly lower rates of wound complications and return trips to the operating room (p=0.03) (Table 2). Overall, 80 % of patients in the NPWT group did not have wound complications versus 68.7% of patients in the DB group, and 4.4% of the NPWT group required a return to the OR versus 6.9% in the DB group (Figure 1).
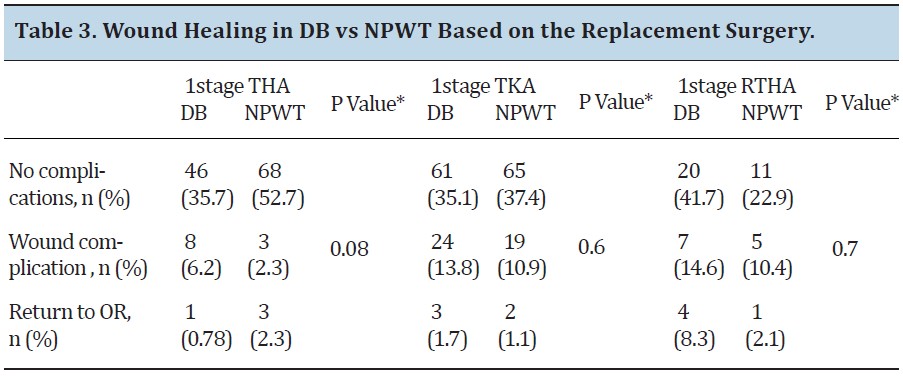
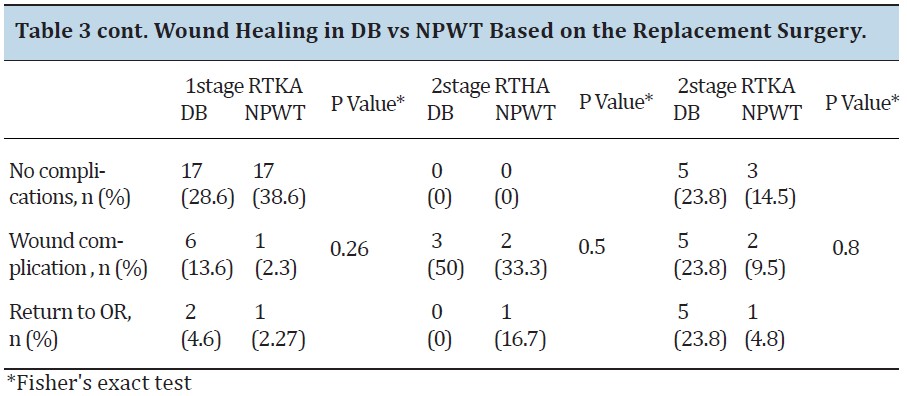
Among primary THA and TKA and revision THA and TKA, a trend for improved wound healing was observed with application of NPWT; however, these did not reach statistical significance. Among all surgery types, the greatest benefit was observed in primary THA. There was 52.7% of NPWT patients who had no complications following primary THA, compared to their 35.7% DB counterparts (p=0.08) (Table 3). A logistic regression model was created to determine the odds ratio of postoperative wound healing associated with wound closure type, while controlling for surgery type, age, BMI, diabetes, and smoking status.
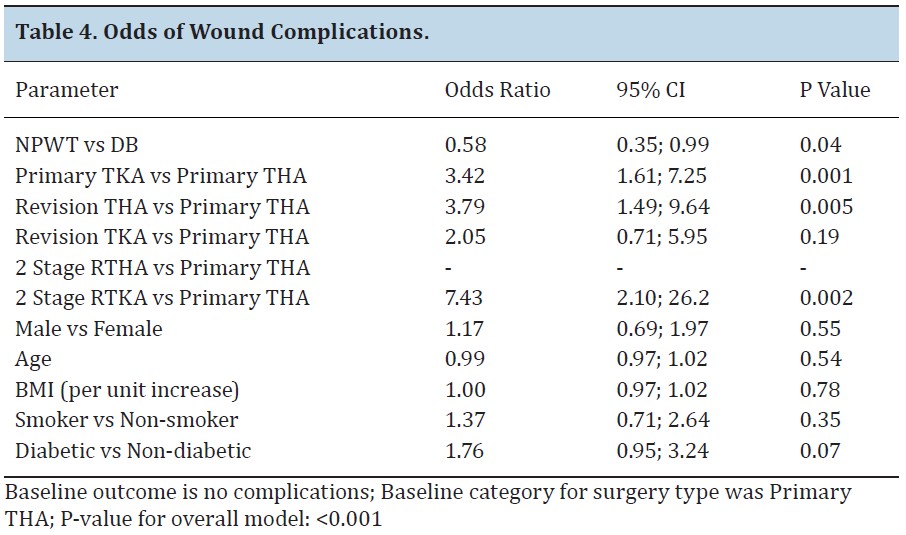
The reference category for the logistic regression model was no wound complication; p<0.05 was accepted as statistically significant. Controlling for all other variables, patients receiving NPWT have 0.58 times the odds of experiencing wound complications as compared to DB (p=0.04) (Table 4). Certain surgical categories carried greater odds of postoperative wound complications. Controlling for all other variables, patients receiving primary TKA have 3.42 times the odds of a wound complication as compared to patients receiving primary THA (p=0.001). After controlling for all other variables, revision THA carried 3.79 times the odds of wound complications as compared to primary THA (p=0.005). Two stage revision TKA carries 7.43 times the risk of wound complications as compared to primary THA (p=0.002) (Table 4). While several patient factors did influence the odds of wound complications (BMI, smoking status, diabetes), no factors achieved statistical significance. There was a trend for diabetic patients as compared to nondiabetic patients to be more likely to have wound complications; however, this did not achieve statistical significance (OR=1.76, p=0.07) (Table 4).
The reference category for the logistic regression model was no wound complication; p<0.05 was accepted as statistically significant. Controlling for all other variables, patients receiving NPWT have 0.58 times the odds of experiencing wound complications as compared to DB (p=0.04) (Table 4). Certain surgical categories carried greater odds of postoperative wound complications. Controlling for all other variables, patients receiving primary TKA have 3.42 times the odds of a wound complication as compared to patients receiving primary THA (p=0.001). After controlling for all other variables, revision THA carried 3.79 times the odds of wound complications as compared to primary THA (p=0.005). Two stage revision TKA carries 7.43 times the risk of wound complications as compared to primary THA (p=0.002) (Table 4). While several patient factors did influence the odds of wound complications (BMI, smoking status, diabetes), no factors achieved statistical significance. There was a trend for diabetic patients as compared to nondiabetic patients to be more likely to have wound complications; however, this did not achieve statistical significance (OR=1.76, p=0.07) (Table 4).

A logistic regression model was also created to determine the odds of return to the operating room. While there was a trend towards decreased return to the operating room in the NPWT group (OR=0.74), this did not achieve statistical significance (p=0.52). Similar to wound complications, certain surgical interventions carried higher odds of return to the operating room. Revision THA was 5.18 more likely to return to the operating room as compared to primary THA (p=0.02). Two stage revision TKA was 21.6 times more likely to return to the operating room as compared to primary THA (p<0.001) (Table 5).
DISCUSSION
The current study demonstrates that within this cohort the use of NPWT results in decreased odds of wound complications as compared to patients closed with DB. This effect was most pronounced within the subgroup of primary THA. There are several published studies describing the benefits of NPWT, but few studies have included as many patients as ours.
Pachowsky et al. [11] investigated the effectiveness of NPWT in the healing of THA and its effect on the occurrence of seroma formation. They studied the results of 19 randomized patients divided into 2 groups. Standard dressings were used in group A, and NPWT was used in group B. Both groups were examined on days 5 and 10, postoperatively. The results showed a significant decrease in the size of the seroma that developed with those dressed with NPWT compared to the control group. Many other studies have shown improved wound healing in both animal and human study models [3,4,12,13,16].
In 2006, Stannard et al. [16] performed a randomized study to evaluate the benefits of NPWT in the healing of surgical incisions and hematomas after a traumatic injury. Forty-four patients were divided into 2 groups, 1 receiving a pressure dressing and the other NPWT. There was a statistically significant difference between the 2 groups with regards to drainage of the wounds. They concluded that the use of NPWT has multiple benefits, including angiogenesis, increased blood flow, and decreased interstitial fluid [16].
Lehner et al. [17] showed the benefit of NPWT as a supportive therapy for treatment of both acute and chronic infections of orthopedic implants. They also showed that early treatment of periprosthetic infections with NPWT was successful, and in some cases the orthopedic implants were able to be left in place rather than explanted [18]. Kelm et al. [19] concluded that vacuum-assisted wound therapy was effective in the treatment of early joint infections when properly used.
DeCarbo et al. [12] described the efficacy of using NPWT in the treatment of lower extremity wounds as well as leading to decreased pain, swelling, and healing time. They concluded that the use of NPWT in the immediate postoperative period was both efficacious and safe in treating high-risk surgical incisions in the lower extremity. Reddix [20] observed a benefit with NPWT used among morbidly obese patients that underwent surgery for acetabular fractures. Incisional wound vacuums used in this group of patients minimized postoperative wound complications including infection and wound dehiscence.
This study is the first to our knowledge to investigate the use of NPWT compared to a DB closure in total joint arthroplasty. Our results are similar to other findings within the literature suggesting superior outcomes with the use of NPWT compared to other methods of wound closure. Although strict inclusion and exclusion criteria were followed, selection bias exists given the retrospective nature of the study. Additionally, this cohort was from a single surgeon and does not reflect the variability that exists between institutions and geographically. Nonetheless, this is a large cohort focusing on differences in postoperative wound complications between DB and NPWT for wound closure. More research is needed to determine if the associated decrease in wound complications with NPWT also translates to decreased postoperative infections. Additionally, more research is needed for patients undergoing revision arthroplasty. A lower odds ratio of wound complications was observed for patients undergoing revision arthroplasty treated with NPWT; however, more data is needed to achieve statistical significance in this subgroup.
The current study demonstrates that within this cohort the use of NPWT results in decreased odds of wound complications as compared to patients closed with DB. This effect was most pronounced within the subgroup of primary THA. There are several published studies describing the benefits of NPWT, but few studies have included as many patients as ours.
Pachowsky et al. [11] investigated the effectiveness of NPWT in the healing of THA and its effect on the occurrence of seroma formation. They studied the results of 19 randomized patients divided into 2 groups. Standard dressings were used in group A, and NPWT was used in group B. Both groups were examined on days 5 and 10, postoperatively. The results showed a significant decrease in the size of the seroma that developed with those dressed with NPWT compared to the control group. Many other studies have shown improved wound healing in both animal and human study models [3,4,12,13,16].
In 2006, Stannard et al. [16] performed a randomized study to evaluate the benefits of NPWT in the healing of surgical incisions and hematomas after a traumatic injury. Forty-four patients were divided into 2 groups, 1 receiving a pressure dressing and the other NPWT. There was a statistically significant difference between the 2 groups with regards to drainage of the wounds. They concluded that the use of NPWT has multiple benefits, including angiogenesis, increased blood flow, and decreased interstitial fluid [16].
Lehner et al. [17] showed the benefit of NPWT as a supportive therapy for treatment of both acute and chronic infections of orthopedic implants. They also showed that early treatment of periprosthetic infections with NPWT was successful, and in some cases the orthopedic implants were able to be left in place rather than explanted [18]. Kelm et al. [19] concluded that vacuum-assisted wound therapy was effective in the treatment of early joint infections when properly used.
DeCarbo et al. [12] described the efficacy of using NPWT in the treatment of lower extremity wounds as well as leading to decreased pain, swelling, and healing time. They concluded that the use of NPWT in the immediate postoperative period was both efficacious and safe in treating high-risk surgical incisions in the lower extremity. Reddix [20] observed a benefit with NPWT used among morbidly obese patients that underwent surgery for acetabular fractures. Incisional wound vacuums used in this group of patients minimized postoperative wound complications including infection and wound dehiscence.
This study is the first to our knowledge to investigate the use of NPWT compared to a DB closure in total joint arthroplasty. Our results are similar to other findings within the literature suggesting superior outcomes with the use of NPWT compared to other methods of wound closure. Although strict inclusion and exclusion criteria were followed, selection bias exists given the retrospective nature of the study. Additionally, this cohort was from a single surgeon and does not reflect the variability that exists between institutions and geographically. Nonetheless, this is a large cohort focusing on differences in postoperative wound complications between DB and NPWT for wound closure. More research is needed to determine if the associated decrease in wound complications with NPWT also translates to decreased postoperative infections. Additionally, more research is needed for patients undergoing revision arthroplasty. A lower odds ratio of wound complications was observed for patients undergoing revision arthroplasty treated with NPWT; however, more data is needed to achieve statistical significance in this subgroup.
There were no conflicts of interest among any of the authors regarding this study. The findings in this study suggest that NPWT is superior with less risk of wound complications compared to DB for wound closure. Wound complications following orthopedic surgery can cause many different problems, and all means available should be utilized to minimize risk. At this time, we continue to utilize NPWT on incisions in the hip and knee for total joint arthroplasty. The benefits shown in the current study could also potentially be applied broadly throughout orthopedic surgical procedures and into other specialties as well.
REFERENCES
[1] Ghomrawi HM, Schackman BR, Mushlin AI. Appropriateness criteria and elective procedure—total joint arthroplasty. N Engl J Med. 2012;367(26):2467-9.
[2] Eggers MD, Fang L, Lionberger DR. A comparison of wound closure techniques for total knee arthroplasty. J Arthroplasty. 2011;26(8):1251-8.
[3] Hill DS, O'Neill JK, Toms A, Watts AM. Pyoderma gangrenosum: A report of a rare complication after knee arthroplasty requiring muscle flap cover supplemented by negative pressure therapy and hyperbaric oxygen. J Plast Reconstr Aesthet Surg. 2011;64(11):1528-32.
[4] Meeker J, Weinhold P, Dahners L. Negative pressure therapy on primarily closed wounds improves wound healing parameters at 3 days in a porcine model. J Orthop Trauma. 2011;25(12):756-61.
[5] Miller AG, Swank ML. Dermabond efficacy in total joint arthroplasty wounds. Am J Orthop (Belle Mead NJ). 2010;39(10):476-8.
[6] Khan RJ, Fick D, Yao F, et al. A comparison of three methods of wound closure following arthroplasty: A prospective, randomised, controlled trial. J Bone Joint Surg Br. 2006;88(2):238-42.
[7] Coulthard P, Esposito M, Worthington HV, van der Elst M, van Waes OJ, Darcey J. Tissue adhesives for closure of surgical incisions. Cochrane Database Syst Rev. 2010;(5):CD004287.
[8] Khurana A, Parker S, Goel V, Alderman PM. Dermabond wound closure in primary hip arthroplasty. Acta Orthop Belg. 2008;74(3):349-53.
[9] Quinn J, Maw J, Ramotar K, Wenckebach G, Wells G. Octylcyanoacrylate tissue adhesive versus suture wound repair in a contaminated wound model. Surgery. 1997;122(1):69-72.
[10] Dragu A, Unglaub F, Schwarz S, et al. Foreign body reaction after usage of tissue adhesives for skin closure: A case report and review of the literature. Arch Orthop Trauma Surg. 2009;129(2):167-9.
[11] Pachowsky M, Gusinde J, Klein A, et al. Negative pressure wound therapy to prevent seromas and treat surgical incisions after total hip arthroplasty. Int Orthop. 2012;36(4):719-22.
[12] DeCarbo WT, Hyer CF. Negative-pressure wound therapy applied to high-risk surgical incisions. J Foot Ankle Surg. 2010;49(3):299-300.
[13] Stannard JP, Atkins BZ, O'Malley D, et al. Use of negative pressure therapy on closed surgical incisions: A case series. Ostomy Wound Manage. 2009;55(8):58-66.
[14] Anagnostakos K, Kelm J, Schmitt E. Indications for use of the V.A.C.-system in the orthopedic surgery. Zentralbl Chir. 2006;131(Suppl 1):S87-92.
[15] Kilic A, Ozkaya U, Sokucu S, Basilgan S, Kabukcuoglu Y. Use of vacuum-assisted closure in the topical treatment of surgical site infections. Acta Orthop Traumatol Turc. 2009;43(4):336-42.
[16] Stannard JP, Robinson JT, Anderson ER, McGwin G,Jr, Volgas DA, Alonso JE. Negative pressure wound therapy to treat hematomas and surgical incisions following high-energy trauma. J Trauma. 2006;60(6):1301-6.
[17] Lehner B, Fleischmann W, Becker R, Jukema GN. First experiences with negative pressure wound therapy and instillation in the treatment of infected orthopaedic implants: A clinical observational study. Int Orthop. 2011;35(9):1415-20.
[18] Lehner B, Bernd L. V.A.C.-instill therapy in periprosthetic infection of hip and knee arthroplasty. Zentralbl Chir. 2006;131(Suppl 1):S160-4.
[19] Kelm J, Schmitt E, Anagnostakos K. Vacuum-assisted closure in the treatment of early hip joint infections. Int J Med Sci. 2009;6(5):241-6.
[20] Reddix RN,Jr, Tyler HK, Kulp B, Webb LX. Incisional vacuum-assisted wound closure in morbidly obese patients undergoing acetabular fracture surgery. Am J Orthop (Belle Mead NJ). 2009;38(9):446-9.
[1] Ghomrawi HM, Schackman BR, Mushlin AI. Appropriateness criteria and elective procedure—total joint arthroplasty. N Engl J Med. 2012;367(26):2467-9.
[2] Eggers MD, Fang L, Lionberger DR. A comparison of wound closure techniques for total knee arthroplasty. J Arthroplasty. 2011;26(8):1251-8.
[3] Hill DS, O'Neill JK, Toms A, Watts AM. Pyoderma gangrenosum: A report of a rare complication after knee arthroplasty requiring muscle flap cover supplemented by negative pressure therapy and hyperbaric oxygen. J Plast Reconstr Aesthet Surg. 2011;64(11):1528-32.
[4] Meeker J, Weinhold P, Dahners L. Negative pressure therapy on primarily closed wounds improves wound healing parameters at 3 days in a porcine model. J Orthop Trauma. 2011;25(12):756-61.
[5] Miller AG, Swank ML. Dermabond efficacy in total joint arthroplasty wounds. Am J Orthop (Belle Mead NJ). 2010;39(10):476-8.
[6] Khan RJ, Fick D, Yao F, et al. A comparison of three methods of wound closure following arthroplasty: A prospective, randomised, controlled trial. J Bone Joint Surg Br. 2006;88(2):238-42.
[7] Coulthard P, Esposito M, Worthington HV, van der Elst M, van Waes OJ, Darcey J. Tissue adhesives for closure of surgical incisions. Cochrane Database Syst Rev. 2010;(5):CD004287.
[8] Khurana A, Parker S, Goel V, Alderman PM. Dermabond wound closure in primary hip arthroplasty. Acta Orthop Belg. 2008;74(3):349-53.
[9] Quinn J, Maw J, Ramotar K, Wenckebach G, Wells G. Octylcyanoacrylate tissue adhesive versus suture wound repair in a contaminated wound model. Surgery. 1997;122(1):69-72.
[10] Dragu A, Unglaub F, Schwarz S, et al. Foreign body reaction after usage of tissue adhesives for skin closure: A case report and review of the literature. Arch Orthop Trauma Surg. 2009;129(2):167-9.
[11] Pachowsky M, Gusinde J, Klein A, et al. Negative pressure wound therapy to prevent seromas and treat surgical incisions after total hip arthroplasty. Int Orthop. 2012;36(4):719-22.
[12] DeCarbo WT, Hyer CF. Negative-pressure wound therapy applied to high-risk surgical incisions. J Foot Ankle Surg. 2010;49(3):299-300.
[13] Stannard JP, Atkins BZ, O'Malley D, et al. Use of negative pressure therapy on closed surgical incisions: A case series. Ostomy Wound Manage. 2009;55(8):58-66.
[14] Anagnostakos K, Kelm J, Schmitt E. Indications for use of the V.A.C.-system in the orthopedic surgery. Zentralbl Chir. 2006;131(Suppl 1):S87-92.
[15] Kilic A, Ozkaya U, Sokucu S, Basilgan S, Kabukcuoglu Y. Use of vacuum-assisted closure in the topical treatment of surgical site infections. Acta Orthop Traumatol Turc. 2009;43(4):336-42.
[16] Stannard JP, Robinson JT, Anderson ER, McGwin G,Jr, Volgas DA, Alonso JE. Negative pressure wound therapy to treat hematomas and surgical incisions following high-energy trauma. J Trauma. 2006;60(6):1301-6.
[17] Lehner B, Fleischmann W, Becker R, Jukema GN. First experiences with negative pressure wound therapy and instillation in the treatment of infected orthopaedic implants: A clinical observational study. Int Orthop. 2011;35(9):1415-20.
[18] Lehner B, Bernd L. V.A.C.-instill therapy in periprosthetic infection of hip and knee arthroplasty. Zentralbl Chir. 2006;131(Suppl 1):S160-4.
[19] Kelm J, Schmitt E, Anagnostakos K. Vacuum-assisted closure in the treatment of early hip joint infections. Int J Med Sci. 2009;6(5):241-6.
[20] Reddix RN,Jr, Tyler HK, Kulp B, Webb LX. Incisional vacuum-assisted wound closure in morbidly obese patients undergoing acetabular fracture surgery. Am J Orthop (Belle Mead NJ). 2009;38(9):446-9.