
Leg Length Discrepancy in a Patient with Ipsilateral Total Knee and Total Hip Arthroplasty
Gaurav S. Sharma, BA; Ronald W. Lindsey, MD
Department of Orthopaedic Surgery and Rehabilitation, University of Texas Medical Branch; Galveston, TX, USA
Corresponding Author:Ronald W. Lindsey, MD, Department of Orthopaedic Surgery and Rehabilitation, University of Texas Medical Branch, 301 University Blvd., Galveston, TX 77555, USA; rlindsey@utmb.edu
DOI: 10.18600/toj.010215
INTRODUCTION
Despite concerted intraoperative attempts to establish equal limb alignment, leg length discrepancy (LLD) remains a frequent complication following elective total hip arthroplasty (THA) [1]. A number of effective intraoperative imaging and clinical limb length techniques have been recommended to minimize this complication; however, all of these assessment modalities have their reported limitations [2,3]. Moreover, the multifactorial nature of the issue of equal leg length has impeded the development of a consensus among hip arthroplasty surgeons on how to best avoid LLD.
We report an unusual case which exemplifies the complexity of this problem in an adult male with ipsilateral total knee arthroplasty (TKA) who experienced LLD following primary THA despite the utilization of recommended imaging and clinical techniques to circumvent this problem.
Despite concerted intraoperative attempts to establish equal limb alignment, leg length discrepancy (LLD) remains a frequent complication following elective total hip arthroplasty (THA) [1]. A number of effective intraoperative imaging and clinical limb length techniques have been recommended to minimize this complication; however, all of these assessment modalities have their reported limitations [2,3]. Moreover, the multifactorial nature of the issue of equal leg length has impeded the development of a consensus among hip arthroplasty surgeons on how to best avoid LLD.
We report an unusual case which exemplifies the complexity of this problem in an adult male with ipsilateral total knee arthroplasty (TKA) who experienced LLD following primary THA despite the utilization of recommended imaging and clinical techniques to circumvent this problem.
CASE REPORT
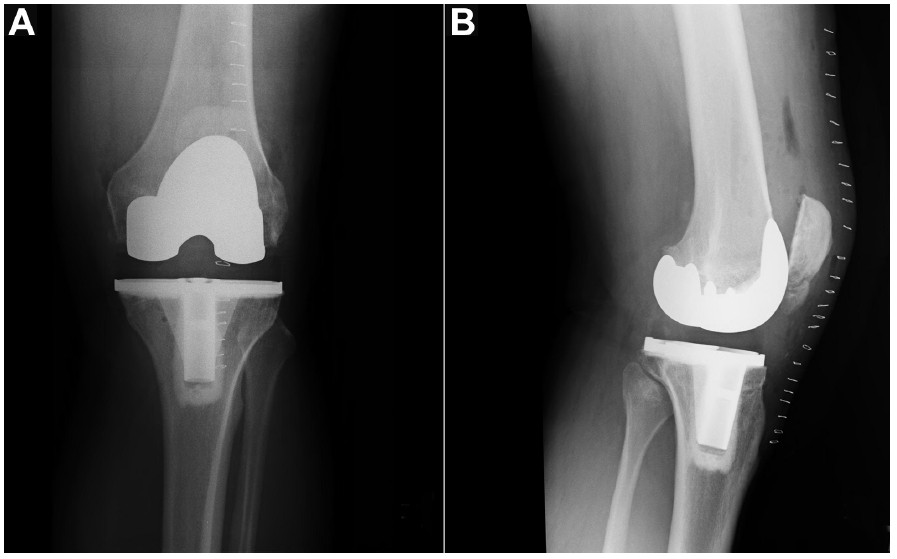
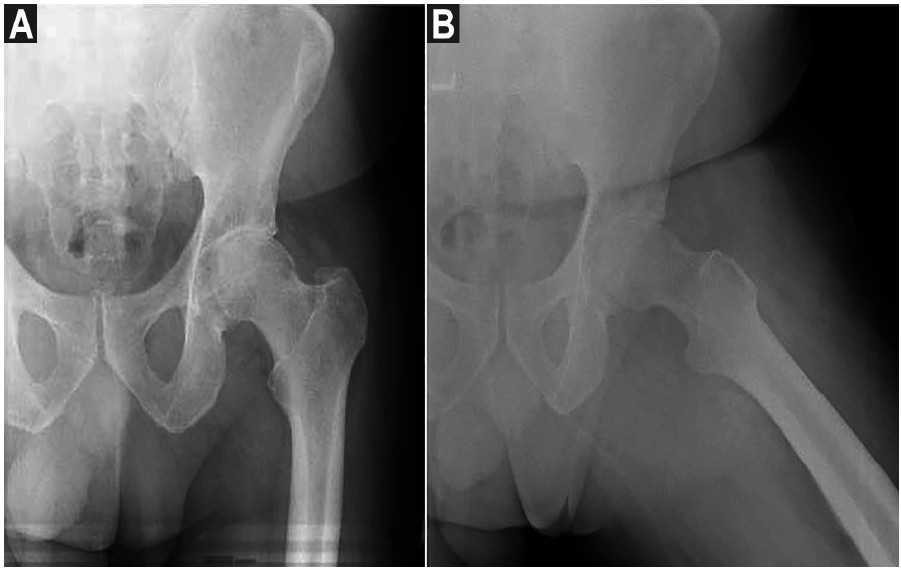
In July 2011, a 59-year-old male presented with severe left hip pain that had progressively increased for approximately 1 year and did not respond to activity modification, cane-assisted ambulation, or nonsteroidal anti-inflammatory medication. His past medical history was unremarkable for an uneventful left TKA 4 years prior, secondary to osteoarthritis (Figure 1). The patient’s functional history included an inability to perform activities of daily living (prolonged standing, walking, or climbing stairs) and his pain persisted during bed rest at night. Physical examination noted decreased active and passive left hip joint motion and severe pain with passive left hip flexion and internal rotation, or resisted left straight leg raise. His leg lengths were symmetric and his gait pattern was normal; however, ambulation was associated with pronounced left groin and greater trochanter pain. Left hip X-rays demonstrated marked degeneration with diffuse joint-space narrowing and anterosuperior acetabulum subchondral sclerosis (Figure 2).
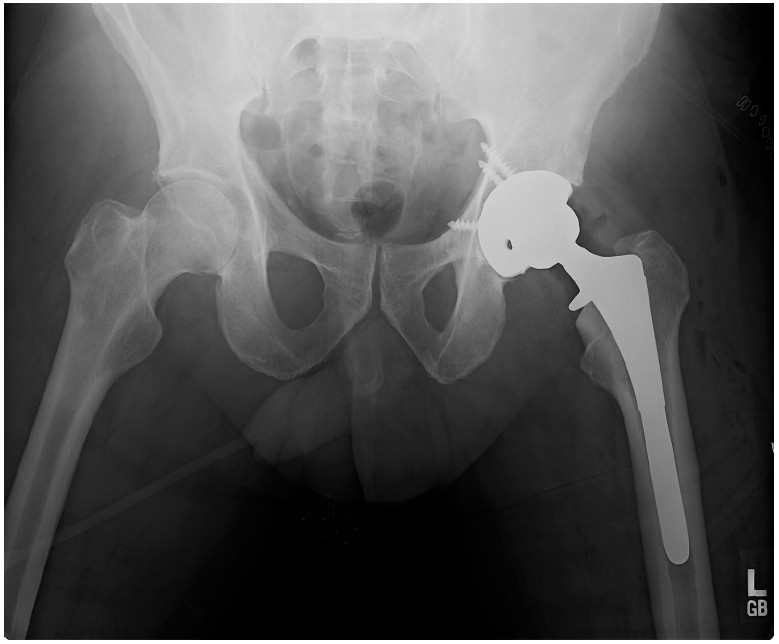
On July 20, 2011 the patient underwent uneventful left total hip arthroplasty through a posterior Kocher-Langenbeck approach, and limb length was established on intraoperative anteroposterior pelvis X-rays by aligning the left lesser trochanter with its right counterpart in accordance to a line extending along the tip of the ischial tuberosities. The leg length established by imaging was also corroborated intraoperatively by the clinical comparison of bilateral femur length with both knees flexed to approximately 60 degrees. Initial postoperative anterolateral pelvis and bilateral hip radiographs 2 weeks postoperatively also confirmed the adequate radiographic length of the patient’s left total hip arthroplasty (Figure 3). Clinically, however, the patient felt that his left leg was longer than the right postoperatively, and subsequent clinical evaluation documented a 3/4-inch leg length discrepancy (left longer than right). Although his preoperative symptoms completely resolved, and the patient quickly returned to a full and unrestricted lifestyle, the LLD was a persistent complaint. The patient was eventually fitted with a 5/8-inch shoe lift to address the LLD.
In July 2011, a 59-year-old male presented with severe left hip pain that had progressively increased for approximately 1 year and did not respond to activity modification, cane-assisted ambulation, or nonsteroidal anti-inflammatory medication. His past medical history was unremarkable for an uneventful left TKA 4 years prior, secondary to osteoarthritis (Figure 1). The patient’s functional history included an inability to perform activities of daily living (prolonged standing, walking, or climbing stairs) and his pain persisted during bed rest at night. Physical examination noted decreased active and passive left hip joint motion and severe pain with passive left hip flexion and internal rotation, or resisted left straight leg raise. His leg lengths were symmetric and his gait pattern was normal; however, ambulation was associated with pronounced left groin and greater trochanter pain. Left hip X-rays demonstrated marked degeneration with diffuse joint-space narrowing and anterosuperior acetabulum subchondral sclerosis (Figure 2).
On July 20, 2011 the patient underwent uneventful left total hip arthroplasty through a posterior Kocher-Langenbeck approach, and limb length was established on intraoperative anteroposterior pelvis X-rays by aligning the left lesser trochanter with its right counterpart in accordance to a line extending along the tip of the ischial tuberosities. The leg length established by imaging was also corroborated intraoperatively by the clinical comparison of bilateral femur length with both knees flexed to approximately 60 degrees. Initial postoperative anterolateral pelvis and bilateral hip radiographs 2 weeks postoperatively also confirmed the adequate radiographic length of the patient’s left total hip arthroplasty (Figure 3). Clinically, however, the patient felt that his left leg was longer than the right postoperatively, and subsequent clinical evaluation documented a 3/4-inch leg length discrepancy (left longer than right). Although his preoperative symptoms completely resolved, and the patient quickly returned to a full and unrestricted lifestyle, the LLD was a persistent complaint. The patient was eventually fitted with a 5/8-inch shoe lift to address the LLD.
DISCUSSION
LLD is the most prevalent complication associated with total hip arthroplasty [1]. LLD, either actual or perceived, has been associated with poor patient functional outcomes and negatively impacts patient satisfaction [1,4]. Although current THA limb length assessment methods frequently employ pre- and intraoperative pelvic radiographs to achieve lower limb length symmetry, no consensus exists in the literature as to how this goal can be reliably accomplished [2,4]. Meermans et al. evaluated the dependability and accuracy of 4 common limb measurement methods reported in 24 studies [2].
When pelvic radiographs were used, they determined that the interteardrop line is more reliable than the bi-ischial line and, in conjunction with the center of the femoral head, should be the preferred pelvis radiographic reference technique.
Also included among the other radiographic leg length measurement methods that have been recommended are full leg standing anteroprsterior (AP) radiographs, intraoperative AP pelvis radiographs, reference pins placed intraoperatively for length measurement, and comparison of the dimensions of resected bone with the dimensions replaced by the prosthesis [2,3]. Another intraoperative clinical limb assessment technique consists of comparing bilateral femur lengths through the sterile drapes with the hips in symmetric degree of flexion. Interestingly, none of these methods, radiographic or clinical, would account for the potential impact of prior lower extremity length abnormalities or surgical interventions. In addition, all of the currently advocated objective THA limb length assessment methods fail to consider the patient’s subjective perception of preoperative leg length symmetry [1].
LLD is the most prevalent complication associated with total hip arthroplasty [1]. LLD, either actual or perceived, has been associated with poor patient functional outcomes and negatively impacts patient satisfaction [1,4]. Although current THA limb length assessment methods frequently employ pre- and intraoperative pelvic radiographs to achieve lower limb length symmetry, no consensus exists in the literature as to how this goal can be reliably accomplished [2,4]. Meermans et al. evaluated the dependability and accuracy of 4 common limb measurement methods reported in 24 studies [2].
When pelvic radiographs were used, they determined that the interteardrop line is more reliable than the bi-ischial line and, in conjunction with the center of the femoral head, should be the preferred pelvis radiographic reference technique.
Also included among the other radiographic leg length measurement methods that have been recommended are full leg standing anteroprsterior (AP) radiographs, intraoperative AP pelvis radiographs, reference pins placed intraoperatively for length measurement, and comparison of the dimensions of resected bone with the dimensions replaced by the prosthesis [2,3]. Another intraoperative clinical limb assessment technique consists of comparing bilateral femur lengths through the sterile drapes with the hips in symmetric degree of flexion. Interestingly, none of these methods, radiographic or clinical, would account for the potential impact of prior lower extremity length abnormalities or surgical interventions. In addition, all of the currently advocated objective THA limb length assessment methods fail to consider the patient’s subjective perception of preoperative leg length symmetry [1].
REFERENCES
[1] Wylde V, Whitehouse SL, Taylor AH, Pattison GT, Bannister GC, Blom AW. Prevalence and functional impact of patient-perceived leg length discrepancy after hip replacement. International Orthopaedics (SICOT). 2009;33:905-9.
[2] Meermans G, Malik A, Witt J, Haddad F. Preoperative Radiographic Assessment of Limb-Length Discrepancy in Total Hip Arthroplasty. Clin Orthop Relat Res. 2011;469:1677-82.
[3] Hofmann A, Bolognesi M, Lahav A, Kurtin S. Minimizing Leg-Length Inequality in Total Hip Arthroplasty: Use of Preoperative Templating and an Intraoperative X-Ray. Am J Orthop. 2008;37(1):18-23.
[4] Clark CR, Huddleston HD, Schoch III EP, Thomas BJ. Leg-Length Discrepancy After Total Hip Arthroplasty. J Am Acad Orthop Surg. 2006;14:38-45.
[1] Wylde V, Whitehouse SL, Taylor AH, Pattison GT, Bannister GC, Blom AW. Prevalence and functional impact of patient-perceived leg length discrepancy after hip replacement. International Orthopaedics (SICOT). 2009;33:905-9.
[2] Meermans G, Malik A, Witt J, Haddad F. Preoperative Radiographic Assessment of Limb-Length Discrepancy in Total Hip Arthroplasty. Clin Orthop Relat Res. 2011;469:1677-82.
[3] Hofmann A, Bolognesi M, Lahav A, Kurtin S. Minimizing Leg-Length Inequality in Total Hip Arthroplasty: Use of Preoperative Templating and an Intraoperative X-Ray. Am J Orthop. 2008;37(1):18-23.
[4] Clark CR, Huddleston HD, Schoch III EP, Thomas BJ. Leg-Length Discrepancy After Total Hip Arthroplasty. J Am Acad Orthop Surg. 2006;14:38-45.